.webp)
A frenectomy is a minor surgical procedure that releases or removes a frenulum — a small fold of tissue connecting one part of the mouth to another. There are three clinically significant frenula: the lingual frenulum (under the tongue), the maxillary labial frenulum (between the upper lip and upper gum), and the mandibular labial frenulum (between the lower lip and lower gum). When a frenulum is too short, too tight, or attached too close to the gum margin, it restricts movement or pulls on tissues in ways that cause functional or structural problems.
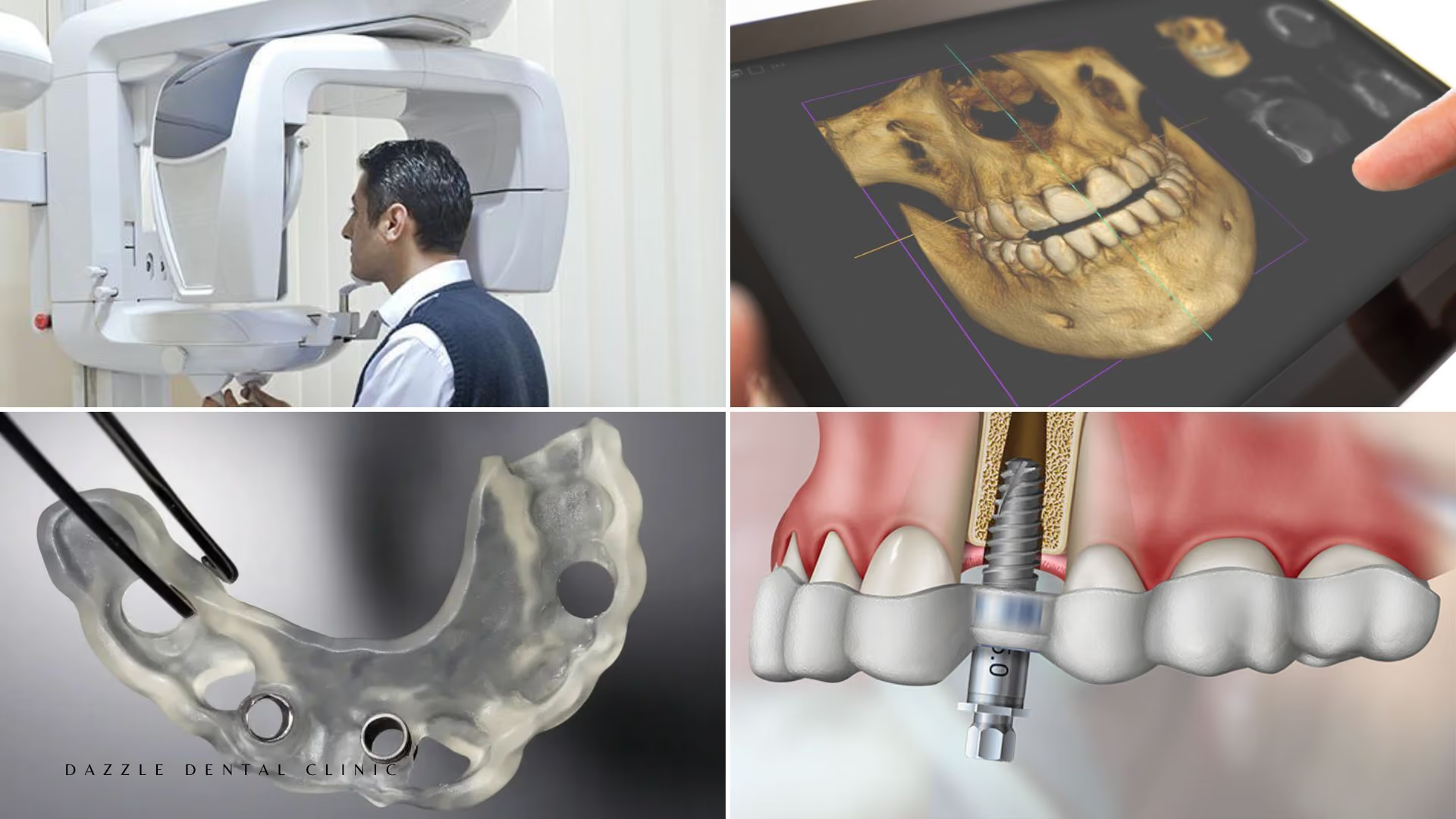
At Dazzle Dental Clinic, frenectomies are performed by the periodontic team using the Fotona Er:YAG laser, which eliminates the need for scalpel incision and sutures in most cases. This is part of the broader periodontic surgical programme that also includes crown lengthening and soft tissue grafting.
Lingual Frenectomy: Tongue Tie (Ankyloglossia)
Ankyloglossia occurs when the lingual frenulum is abnormally short or has a low attachment point, restricting tongue elevation and lateral movement. Clinical impact varies with severity:
In infants: restricted tongue mobility impairs latch during breastfeeding, causing poor milk transfer and maternal nipple pain. Lingual frenectomy (frenotomy) in this age group is a simple 30-second procedure with local anaesthetic cream — no injection required in newborns — and produces immediate improvement in latch in published case series.
In children: speech sound production that requires tongue elevation (L, N, T, D, Th, R) may be affected by severe ankyloglossia. Whether tongue tie is the cause of a specific child’s speech difficulty requires assessment by a speech therapist before frenectomy is planned — not all speech difficulties in children with tongue tie are caused by the tongue tie.
In adults: generalised tongue restriction may limit intraoral hygiene access behind lower incisors, contribute to snoring by limiting tongue posture, and create discomfort during extended speech or singing. Adult lingual frenectomy is more involved than the infant procedure and is performed under local anaesthesia at Dazzle using the Fotona laser.
Maxillary Labial Frenectomy: Upper Lip Tie and Diastema
The maxillary labial frenulum connects the inner surface of the upper lip to the gum between the upper central incisors. When this frenulum is prominent and attaches close to or at the gum margin between the centrals, it can: cause a midline diastema (gap between the upper front teeth) that does not close with orthodontic treatment because the frenulum prevents the teeth from moving fully together; contribute to upper lip restriction that limits lip mobility and, in infants, impairs breastfeeding lip seal.
Frenectomy is not indicated simply because a maxillary frenulum is visible — most labial frenula are normal anatomical structures. The indication is: a diastema that orthodontic treatment cannot fully close without frenectomy, or a low attachment causing gum blanching and recession in the interdental area. Gum recession in the interdental area should be assessed in the context of a full periodontal assessment.
The Fotona Laser Procedure at Dazzle
Laser frenectomy at Dazzle uses the Fotona Er:YAG laser in MST (micro-smooth technique) mode. Local anaesthetic topical gel is applied for soft tissue procedures; injection may be needed for lingual frenectomies in adults. The laser vaporises the frenulum tissue with precision, coagulating blood vessels simultaneously — the procedure is essentially bloodless. No scalpel, no sutures. Post-operative discomfort: mild, 1–3 days. Healing: 1–2 weeks. Patients can eat soft foods immediately.
FAQs
Q1: How do I know if my child has tongue tie?
Characteristic signs in infants: clicking sound during breastfeeding, poor weight gain, maternal nipple pain, short feeding sessions followed by hunger. In children: specific speech sound difficulties (sounds requiring tongue elevation), visible restriction when the child tries to stick the tongue out past the lower teeth. A clinical assessment at Dazzle evaluates tongue mobility using the Hazelbaker or Kotlow classification scales.
Q2: Will frenectomy fix my child’s speech?
In cases where tongue mobility restriction is the primary cause of the speech difficulty, frenectomy combined with speech therapy produces improvement. Frenectomy alone without speech therapy is less effective for established speech patterns — the release needs to be followed by exercises and, in older children, professional speech therapy. This is why speech therapy assessment before frenectomy is the recommended sequence.
Q3: Is frenectomy painful?
Laser frenectomy for adults under local anaesthesia: no pain during the procedure. Post-operatively: mild soreness for 1–3 days, managed with NSAIDs. For infant frenotomy: brief discomfort during the procedure and typically no post-operative distress; babies usually feed within minutes of the procedure.
Q4: Can a frenectomy be combined with orthodontic treatment?
Yes — this is the standard sequence for diastema closure. The frenectomy is performed either before or at the end of orthodontic treatment (timing depends on the specific case). If performed before braces, the frenulum scar tissue must fully mature (3–6 months) before the centrals are moved fully together to prevent relapse. If performed at the end of orthodontic treatment, it removes the obstacle that was preventing the centrals from approximating fully, after which a retainer maintains the closure.