.webp)
The clinical argument for multi-disciplinary planning in dentistry is straightforward: treatment outcomes in complex cases are determined not only by how well each individual procedure is executed, but by whether the procedures were planned in the right sequence, with the right endpoints, by the right specialists before any work begins. A restorative plan that does not account for periodontal disease creates restorations that fail at the margin. An implant plan that does not account for the prosthetic outcome places implants in positions that make the final crown anatomically difficult. A smile makeover that does not address jaw alignment first creates veneers over teeth that will move.
At Dazzle Dental Clinic, complex cases involving more than one specialist domain are assessed and planned collaboratively before the treatment plan is presented to the patient. This is not a marketing claim — it is a clinical workflow with specific implications for outcomes.
What Multi-Disciplinary Planning Involves in Practice
For a straightforward case — a patient needing a single crown on a tooth with adequate periodontal health — one clinician makes all necessary decisions and the treatment is uncomplicated. For a complex case, the clinical picture spans multiple domains simultaneously. A patient presenting for full-mouth rehabilitation with implants may have: active periodontal disease requiring treatment before implants; bone deficiency requiring augmentation before or at implant placement; a prosthetic plan that determines where the implants must be positioned; and a gum architecture that needs correction before the final crowns are made.
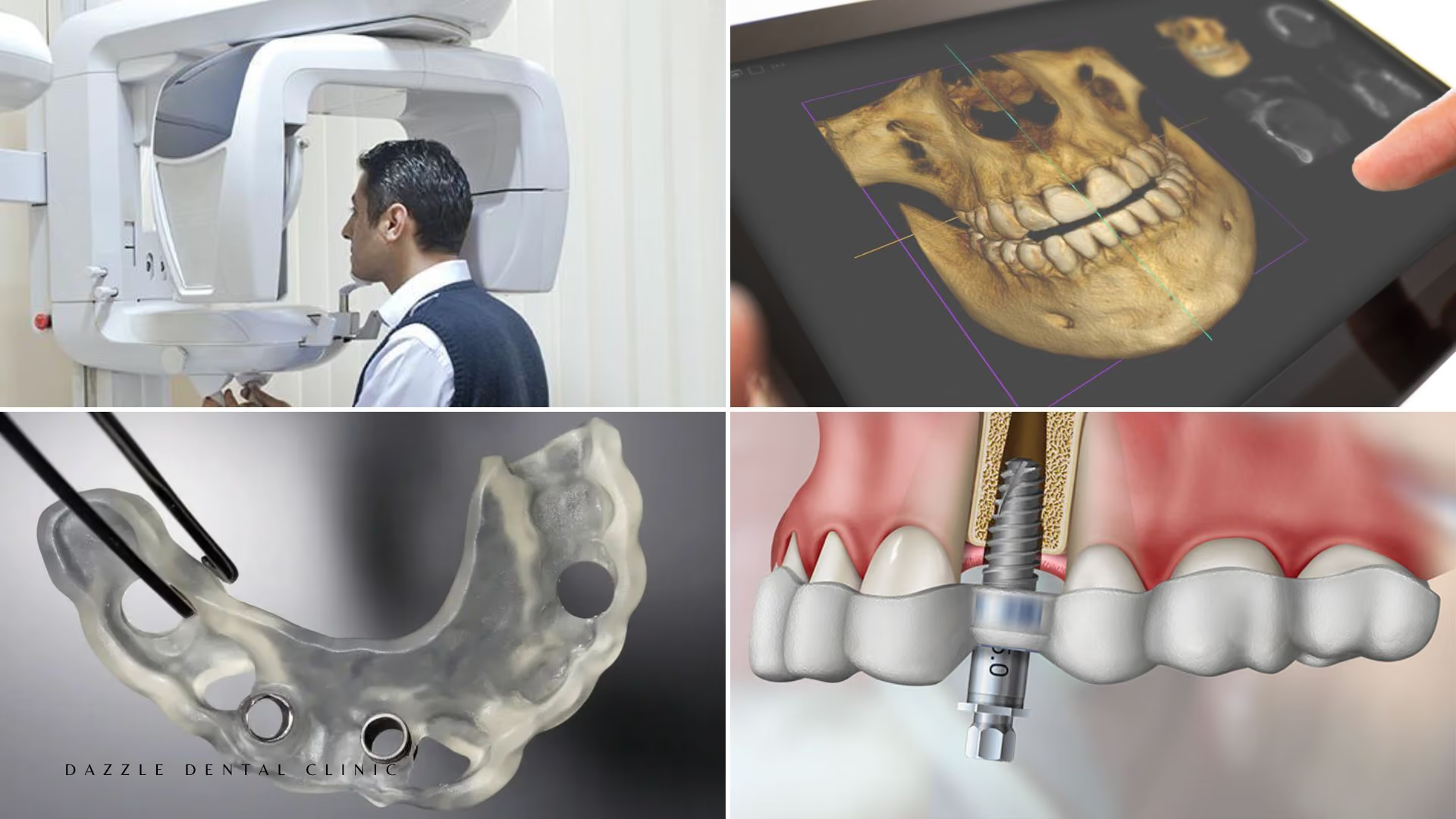
Collaborative planning at Dazzle: the implantologist, prosthodontist, and periodontist review the CBCT data and diagnostic imaging simultaneously. They agree on the treatment sequence, the prosthetic design, the implant positions, the graft approach, and the gum correction timing before any work begins. The patient receives a single integrated treatment plan, not a sequence of referrals.
How Collaborative Planning Changes Specific Outcomes
Implant position and prosthetic outcome: The prosthodontist's input on the final crown or bridge position determines where the implant must be placed — not just where bone is available. An implant placed purely on bone availability without prosthodontic guidance may end up in a position that makes the crown difficult to clean, aesthetically compromised, or functionally unstable. Prosthetically guided implant planning is the clinical standard; it requires prosthetic input at the planning stage, not after placement.
Periodontal treatment sequencing: At Dazzle, no restorative or implant work begins while active periodontal disease is present. The periodontist assesses periodontal status, treats active disease, and confirms periodontal stability before the restorative phase begins. Crowns placed on periodontally unstable teeth fail at the margin as the gingival level drops. The sequence matters.
Gum line correction timing: In smile makeover cases involving both gum contouring and veneers, the gum correction is done first and allowed to heal (6–8 weeks for crown lengthening, 2–4 weeks for laser contouring) before veneer preparation is begun. Reversing this sequence produces veneers with margins set to a gum level that then changes.
The In-House Advantage
All specialists at Dazzle are available in-house. This means the collaborative case discussion is a direct conversation between clinicians who know each other's work, share the same patient records, and are available for intra-procedure consultation if needed. A periodontist who identified a bone defect during crown lengthening can communicate directly with the implantologist planning that site — the information is not filtered through referral letters.
FAQs
Q1: Will I be seen by multiple dentists for a complex case?
Yes, where the case spans multiple specialist domains. Each specialist is responsible for their component. The treatment plan is integrated so that the specialists' work is coordinated rather than sequential-and-independent. For routine cases, one clinician manages the case entirely. This approach is especially valuable for full-mouth rehabilitation and complex implant treatment requiring multiple specialists.
Q2: Does multi-specialist treatment cost more?
The cost reflects the procedures and specialist consultations involved. For complex cases, having specialists involved from the planning stage reduces the cost of later corrections — a failed bone graft that needed adjustment, an implant that required prosthetic reworking, or a veneer that had to be remade after gum healing changed the margin. The cost of collaborative planning is typically lower than the cost of uncoordinated sequential treatment with corrections.
Q3: How long does multi-disciplinary treatment planning take?
The initial assessment is 45–60 minutes. The imaging review and case discussion between specialists typically occurs within 2–3 working days. The treatment plan is presented to the patient at a second appointment where the sequence, timeline, and costs are discussed fully before any treatment begins.
Q4: Can I bring a second opinion to the collaborative planning appointment?
Yes. Patients are welcome to bring their own records, previous treatment histories, and imaging from other clinicians. The collaborative assessment at Dazzle incorporates all available information rather than disregarding prior clinical history.