.webp)
Bone loss exists on a spectrum. “Severe bone loss” can mean the posterior alveolar ridge is resorbed but the anterior bone is intact — in which case conventional All-on-4 may still be viable with appropriate angulation. Or it can mean the entire alveolar arch has resorbed, the sinus floor is at the crest level, and no conventional implant position achieves adequate primary stability — in which case zygomatic and/or pterygoid implants are required. The clinical approach to extreme bone loss must be calibrated to the specific anatomy, not to a categorical rule.
Mapping the Spectrum of Bone Loss to Clinical Approaches
Moderate posterior atrophy with intact anterior ridge: Conventional All-on-4 — the two angled posterior implants are placed with their apices in the denser bone anterior to the sinus; the two anterior implants engage what remains of the anterior ridge. This is the most common full-arch configuration and does not require zygomatic or pterygoid implants.
Moderate-to-severe posterior atrophy with compromised anterior: Angled All-on-4 may achieve marginal primary stability but falls below the 35 Ncm threshold at one or more posterior sites. Options: (1) proceed with conventional implants at the sites that do achieve threshold, defer loading at sites that don’t; (2) add zygomatic implants at the sites where conventional stability is inadequate. The intraoperative torque measurement determines which path is taken.
Severe bilateral posterior atrophy, sinus floor at or near crest: Conventional All-on-4 is not viable posteriorly. Two zygomatic implants (one per side) replace the conventional posterior implants. Two conventional anterior implants remain where the anterior ridge permits. This four-implant configuration — two zygomatic + two anterior — is the most common zygomatic configuration at Dazzle. For full detail on this candidacy assessment, see the zygomatic candidate assessment article.
Severe atrophy across the full arch including anterior: Even the anterior ridge cannot provide stable conventional implant anchorage. Four zygomatic implants (quad-zygoma), two per side at different angles providing anterior and posterior support, with no conventional implants. This is the most extensive configuration and is reserved for the most severe cases.
Posterior atrophy requiring extended AP spread: Either of the above configurations, with pterygoid implants added to extend the distal anchor point and increase AP spread. Used when the planned cantilever would otherwise be clinically unacceptable.
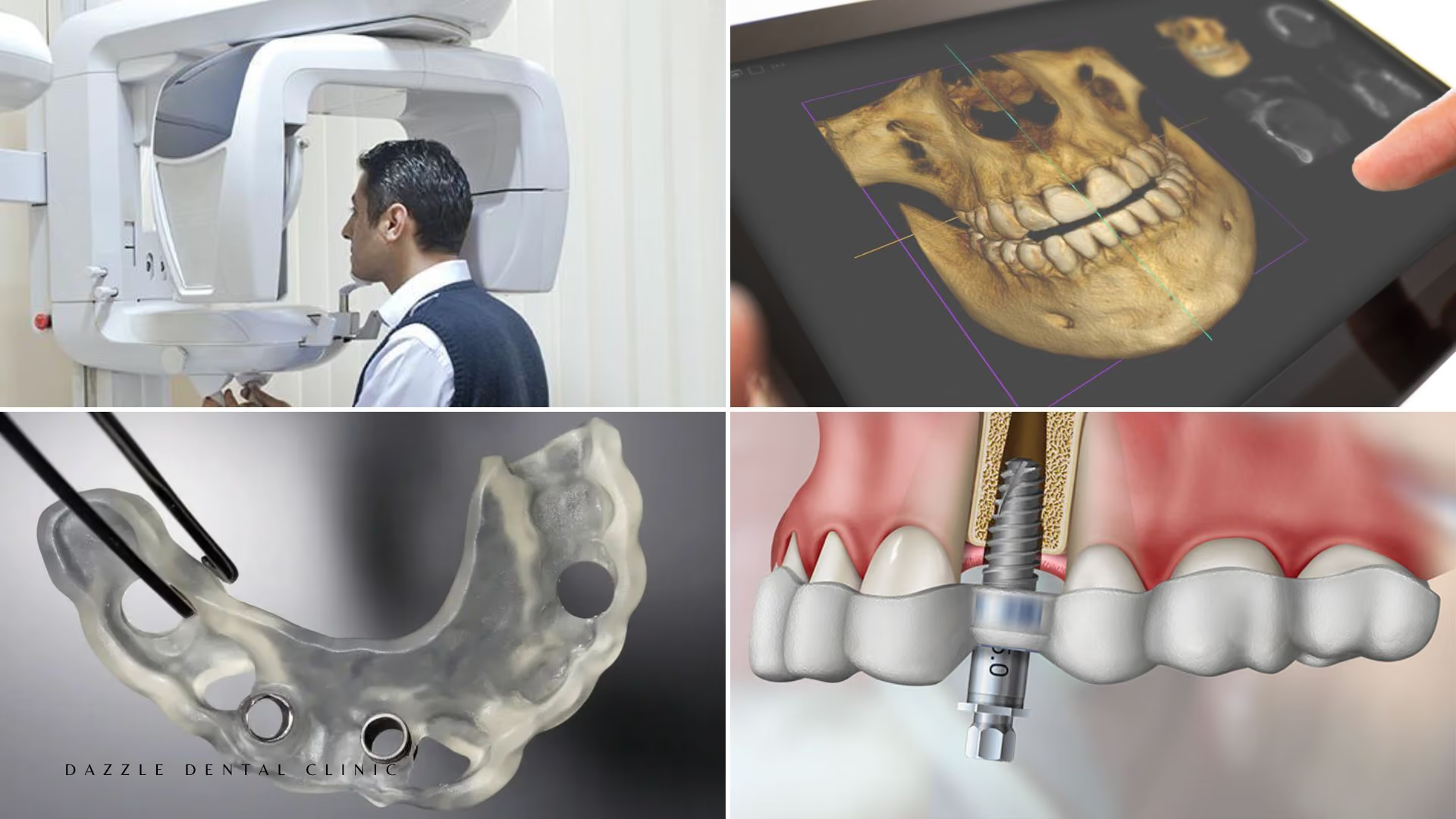
How Bone Loss Severity Is Measured
CBCT quantifies bone height and width at each proposed implant site in millimetres. The key thresholds: a minimum of 8–10mm bone height and 5–6mm width is generally required for conventional implant placement. In the posterior maxilla, the distance from the alveolar crest to the sinus floor defines available height. When this is less than 5mm at all posterior sites and cannot be addressed by angulation, zygomatic implants are indicated.
At Dazzle, every full-arch case begins with CBCT analysis. The specific bone measurements at each planned site are reviewed before the treatment plan is presented, and the configuration recommendation is based on these measurements rather than on a blanket policy.
What Patients in This Situation Can Realistically Expect
Patients with extreme bone loss who receive zygomatic or zygomatic + pterygoid implants can expect: same-day provisional fixed bridge; soft diet for 6–8 weeks; final prosthesis at 4–6 months; published 10-year implant survival of 95–98% in experienced hands; and the same functional and aesthetic outcome as conventional full-arch patients — a fixed bridge that does not come out and supports normal eating and speech.
FAQs
Q1: I have been told I have ‘extreme bone loss’. What does that mean specifically?
Without a CBCT report, “extreme bone loss” is a clinical description, not a precise measurement. Ask the clinician: what is the measured bone height at the proposed implant sites? What is the distance from the alveolar crest to the sinus floor at the posterior sites? These numbers determine what is and is not possible. If a clinician cannot provide these measurements, they have not assessed the case with sufficient precision.
Q2: Do zygomatic implants restore the same function as conventional implants?
Yes. The patient experience — eating, speaking, cleaning, aesthetics — is identical between zygomatic and conventional full-arch bridges. The anchorage is different; the prosthetic outcome is the same.
Q3: Is bone grafting ever combined with zygomatic implants?
Sometimes, for localised anterior deficiencies where the anterior ridge needs augmentation to support the two conventional anterior implants. Socket preservation grafting at the time of extraction is also standard when teeth are removed at the same surgical session. Major sinus augmentation is not combined with zygomatic implants — the zygomatic approach eliminates the need for it.
Q4: How do I compare treatment costs across clinics offering zygomatic implants?
The relevant comparison is: what implant system is being used (Nobel Zygoma vs non-published systems); what is included in the quoted cost (provisional bridge, final prosthesis material, CBCT, follow-up appointments); and what is the prosthesis material for the final bridge (zirconia vs acrylic). Comparing headline prices without these details does not produce a meaningful comparison.