.webp)
The accuracy of an implant’s position in bone — its depth, angulation, mesiodistal location, and proximity to anatomical structures — directly determines long-term outcomes: the fit of the prosthesis, the distribution of occlusal forces, peri-implant bone stability, and whether adjacent nerves and the sinus floor were respected during placement. These outcomes are not determined by technique alone; they are determined by the quality of planning that precedes the surgical appointment.
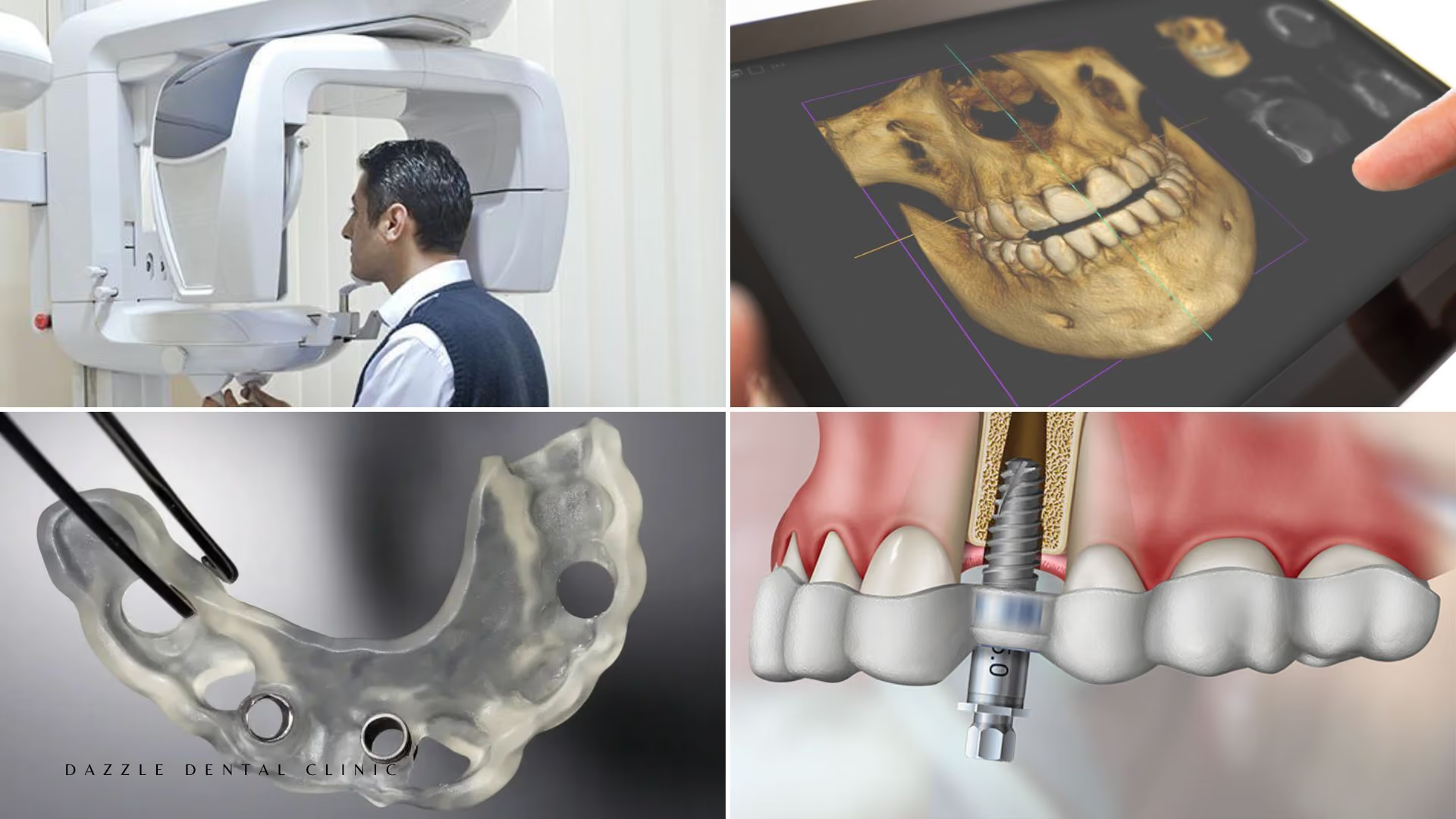
Digital dentistry at Dazzle Dental Clinic means a continuous digital chain from CBCT imaging through virtual surgical planning to guided implant placement and in-house prosthesis fabrication. Here is what each component actually does.
CBCT Imaging: Why 3D Planning Is Non-Negotiable for Full-Arch Cases
A panoramic X-ray reveals bone height in two dimensions. It cannot measure bone width, cannot accurately localise the inferior alveolar nerve in three dimensions, and cannot assess bone density. For a full-arch All-on-4 or All-on-6 case where posterior implants are angled at 30–45 degrees, the three-dimensional bone architecture at each proposed placement site is critical planning information. Radiation dose for a dental CBCT: 20–100 μSv — comparable to 2–3 days of background radiation. The diagnostic value for implant planning far exceeds this exposure.
At Dazzle, CBCT imaging is part of every full-arch implant workup. From the three-dimensional dataset, the implantologist measures bone height, width, and density at each planned site; maps the exact positions of the inferior alveolar nerve canal, mental foramen, and sinus floor; and determines the implant diameter, length, and angulation for each fixture before entering the operating room.
Virtual Surgical Planning: Designing the Case Before the First Incision
The CBCT data is imported into implant planning software (coDiagnostiX or equivalent) where the complete surgical procedure is designed virtually. Every implant is positioned to: maximise bone contact at the chosen diameter and length; achieve the AP spread (anterior-posterior distribution across the arch) necessary for prosthetic stability; maintain safe margins from anatomical structures; and produce abutment emergence angles that support the planned prosthetic bridge design. The virtual plan integrates prosthetic planning with surgical planning — implants are positioned from the prosthesis backward, not placed first and accommodated afterward.
Digital Smile Design: Linking Aesthetics to the Surgical Plan
For cases where the aesthetic outcome is a central patient priority, Digital Smile Design (DSD) overlays the planned tooth positions and gum contour onto the patient’s facial photographs and intraoral scans. The patient previews the planned result before any preparation or surgery begins. At Dazzle, DSD is used for appropriate full-arch and cosmetic cases as part of the pre-treatment workflow. The approved aesthetic plan informs the virtual surgical plan — ensuring the implant positions will support the planned prosthesis geometry.
3D-Printed Surgical Guides: Executing the Plan with Precision
The surgical guide (stent) is fabricated from the virtual plan — a custom device printed on the in-house Asiga Max 3D printer that fits over the patient’s gum or remaining teeth and physically constrains the surgical drill to the planned position, angulation, and depth. This eliminates the freehand interpretation step. Published accuracy: apex deviation under 1mm from planned position; angular deviation under 2°. The clinical consequences of this precision: nerve structures are protected because the depth stop on the guided drill prevents overdrilling; implant positions match the virtual plan; the prosthetic team receives implants where they anticipated them.
At Dazzle, guided surgery is standard for all full-arch implant cases and for single implants in proximity to critical anatomical structures. Freehand full-arch placement is not the approach used.
In-House Laboratory: Completing the Digital Chain
The final prosthesis is fabricated from the intraoral scan taken after osseointegration, designed in CAD software, and milled from solid zirconia blocks in the in-house Amann Girrbach unit. The clinical team and laboratory technicians work on the same case directly — no external lab communication gap. For international patients, the provisional bridge is pre-fabricated before surgery from the pre-surgical scan, ready to be placed the day of surgery without waiting for external laboratory turnaround.
FAQs
Q1: Does guided surgery guarantee perfect placement?
Guided surgery significantly reduces placement deviation. Under 1mm apex deviation and under 2° angular deviation are the published accuracy benchmarks. Guide fit, bone density variation, and surgeon technique still contribute to the final outcome. Guided surgery eliminates most of the freehand error; it does not make the surgeon irrelevant.
Q2: Is CBCT imaging safe?
Yes. The effective dose (20–100 μSv for a dental CBCT) is approximately equivalent to 2–3 days of natural background radiation. Medical chest CT delivers approximately 7,000 μSv — roughly 70–350 times higher than a dental CBCT. The diagnostic benefit for implant planning is well established and the radiation risk is negligible in context.
Q3: Can I see a simulation of my planned smile before surgery?
Yes, for appropriate cases. DSD produces a visual preview of the planned prosthesis integrated with your facial photographs. This is discussed at consultation and incorporated into the pre-treatment workflow where clinically relevant.
Q4: Do all clinics offering All-on-4 use guided surgery?
No. Guided surgery requires CBCT imaging, planning software, and guide fabrication — steps some clinics skip to reduce cost or time. The clinical outcomes differ measurably in implant position accuracy and nerve protection. Whether guided surgery is included is a reasonable question to ask any clinic before committing to treatment.