.webp)
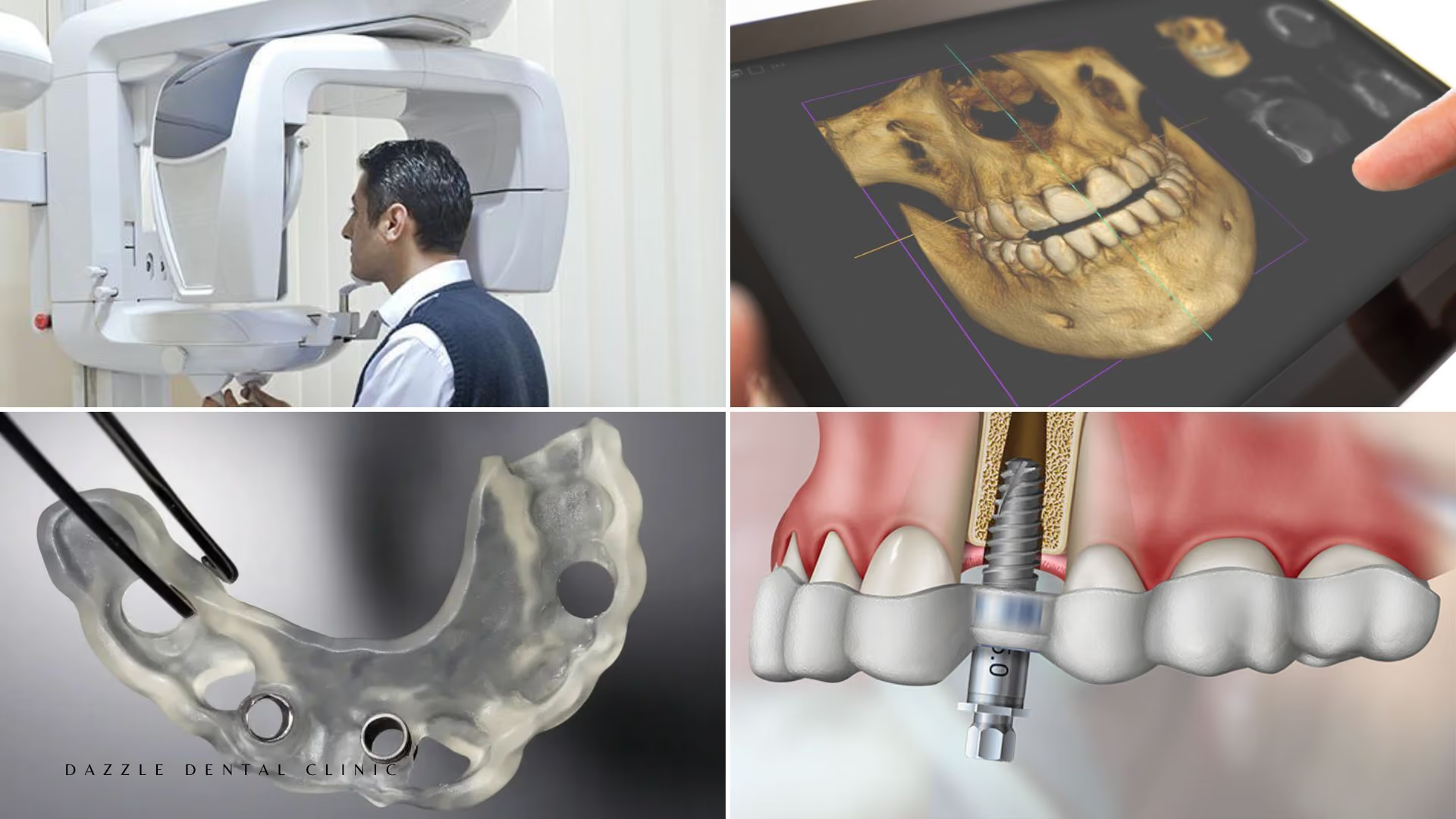
Same-day teeth in complex cases require more than high primary stability — they require a surgical plan that anticipates anatomical challenges before the first incision, and the clinical flexibility to adapt intraoperatively when anatomy deviates from the plan. This article covers how same-day implant loading is achieved for patients with severely atrophic bone, failed implants, or medical complexity.
What Makes a Case "Complex"
In full-arch implant surgery, complexity is defined by the challenges that increase the probability of failing to achieve the primary stability threshold required for immediate loading. The most common sources of complexity at Dazzle: severe posterior maxillary atrophy requiring zygomatic or pterygoid implants; failed previous implants with sites requiring regeneration before re-implantation; poor bone quality (Type III-IV throughout) where standard thread design cannot achieve 35 Ncm insertion torque; and medical factors (controlled diabetes, smoking history) that compress the margin for error.
The Role of Zygomatic and Pterygoid Implants in Complex Cases
When the posterior maxilla lacks adequate bone for conventional or tilted implants, zygomatic and pterygoid implants provide anchorage in dense extra-alveolar bone. Both engage cortical bone outside the alveolar ridge — the zygomatic implant in the cheekbone, the pterygoid implant in the sphenoid pterygoid plates. Both avoid the sinus. Both allow same-day loading.
The combination most commonly used at Dazzle for severe maxillary atrophy: two zygomatic implants (one per side) + two anterior conventional implants. Where AP spread from two zygomatic implants is insufficient, pterygoid implants add posterior anchorage. For the full clinical detail on this approach, see our zygomatic and pterygoid guide.
Primary Stability in Compromised Bone
In soft bone, primary stability is the key variable. The strategies used at Dazzle to achieve threshold torque in compromised bone: implant system selection — progressive thread design implants (Nobel Active, MegaGen AnyRidge) achieve higher torques in soft bone through bone condensation; under-drilling the osteotomy condenses bone laterally; implant diameter and length are maximised within anatomical limits. See our primary stability guide for the clinical thresholds.
Planning for Contingencies
Complex cases require explicit contingency planning communicated to the patient before surgery. At Dazzle, every complex case is discussed with: the expected protocol; the contingency if threshold stability is not achieved; and what that means for the provisional timeline. Patients are not surprised by a delayed loading decision if anatomy requires it. The surgical plan includes alternative implant positions, alternative implant systems, and the decision tree for switching from immediate to staged loading intraoperatively. For our full All-on-4 treatment overview, see the dedicated page.
FAQs
Q1: How do I know if my case is too complex for same-day teeth?
The CBCT assessment determines this. At Dazzle, we provide a specific assessment of your anatomy, the proposed implant positions, the expected insertion torques for those positions, and the probability that same-day loading will be achievable. "Complex" does not mean same-day loading is impossible — it means more planning and contingency preparation is required.
Q2: Does zygomatic implant surgery involve more recovery than conventional All-on-4?
The recovery is longer. Zygomatic implants pass through more soft tissue than conventional implants. Swelling is typically greater (peaking at 72-96 hours rather than 48-72 hours) and resolves over 10-14 days. Most patients are comfortable for travel at day 6-7.
Q3: Can teeth still be placed the same day with zygomatic implants?
Yes. At Dazzle, same-day provisional bridges are placed on zygomatic implant cases where all implants achieve threshold stability. The difference from conventional cases is that zygomatic implants almost always achieve adequate primary stability due to the dense cortical bone engagement — making immediate loading more reliably achievable, not less, in severe atrophy cases.
Q4: Why is the second visit necessary — can the final bridge not be placed at surgery?
The final bridge requires osseointegration to be confirmed before it is fitted. The provisional bridge is the insurance: if an implant fails during healing, it is managed before the final bridge is fabricated, saving the cost and time of remaking a high-quality final restoration.