.webp)
An apicoectomy is a minor surgical procedure performed when a tooth with a root canal has persistent infection at the apex (tip) of the root that non-surgical retreatment cannot resolve. It is not an alternative to root canal treatment — it is performed on teeth that already have root canal treatment, when that treatment has failed to eliminate the periapical pathology.
At Dazzle Dental Clinic, apicoectomy is performed by an experienced periodontist rather than a general dentist, because the procedure requires precise soft tissue management, microsurgical technique, and the ability to assess and seal the root end under magnification. The outcome data for apicoectomy correlates directly with the operator’s surgical skill and the use of surgical microscopy.
When Apicoectomy Is Indicated
Apicoectomy is not the first response to root canal failure. The sequence is: first, assess whether non-surgical retreatment (re-root canal treatment) can address the failure. Retreatment resolves most root canal failures and is the less invasive option where technically feasible. Apicoectomy is indicated when:
Non-surgical retreatment is not possible because: the canal is blocked by a post or separated instrument that cannot be retrieved; the canal system is calcified and not accessible by conventional means; a previous retreatment has already failed to resolve the periapical lesion.
Non-surgical retreatment is possible but the source of failure is apical rather than coronal: a root fracture at or near the apex; a persistent apical cyst rather than a granuloma (cysts have an epithelial lining that does not resolve with canal disinfection); apical transportation or perforation from the original root canal that cannot be managed from within the canal.
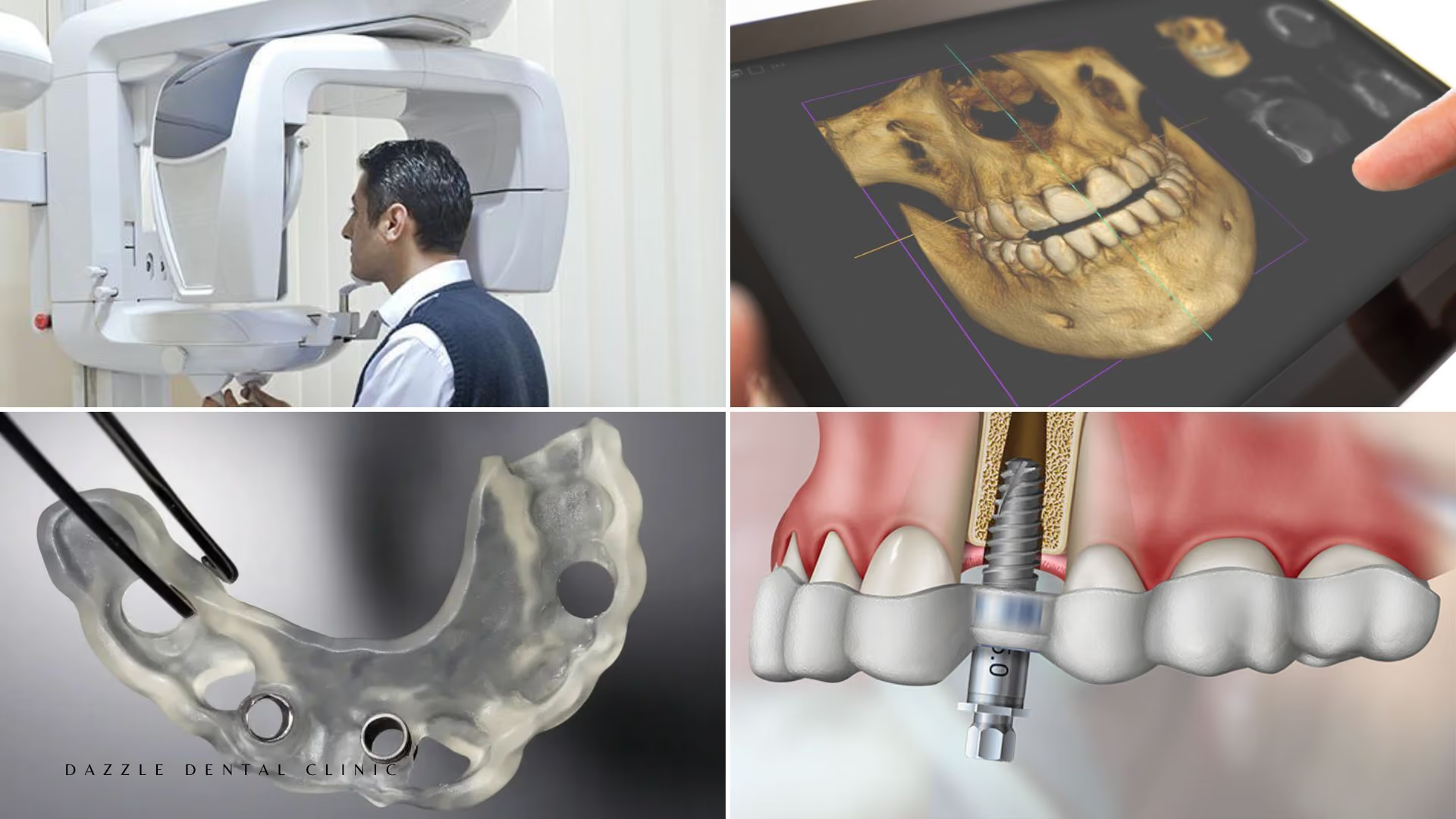
In these cases, direct surgical access to the apex allows the infected root tip to be removed (typically 2–3mm of root length) and the root end to be sealed from outside. For complex cases, a CBCT scan guides surgical planning.
The Procedure at Dazzle
Pre-surgical assessment: CBCT imaging is used for all apicoectomy cases at Dazzle to define the three-dimensional relationship of the root apex to adjacent structures — the inferior alveolar nerve in the mandible, the maxillary sinus floor for upper premolars and molars, and the adjacent root apices. Periapical films alone are insufficient for surgical planning in complex cases.
Anaesthesia: Local anaesthesia. The procedure is performed without pain. Sedation is available for anxious patients.
Surgical access: A flap is elevated in the attached gingiva adjacent to the affected tooth, exposing the outer bone surface at the root apex. A small osteotomy (bone window) is made to expose the root tip.
Root-end resection: 2–3mm of the root tip is removed with a surgical bur. The resected root face is inspected under magnification (surgical microscope or loupes) to confirm the canal anatomy and identify any cracks, fins, or accessory canals that the original canal preparation may have missed.
Root-end preparation and filling: A retrograde preparation is made using ultrasonic tips to create a cavity in the resected root face. This cavity is filled with MTA (mineral trioxide aggregate) or Biodentine — biocompatible calcium silicate cements that seal the root end from the apical direction and support periapical healing.
Flap repositioning and suturing: The flap is repositioned and sutured. Resorbable sutures are standard; patients return for suture removal or sutures dissolve at 7–10 days.
Published Success Rates
Published apicoectomy success rates in the contemporary microsurgical literature: 85–95% periapical healing at 2–4 years follow-up. This compares favourably with non-surgical retreatment (70–85% success) in cases where both options are viable. The key determinant of success is complete periapical healing confirmed radiographically at 6 months and 1 year post-surgery.
FAQs
Q1: How long does the apicoectomy procedure take?
30–90 minutes depending on the tooth location, root anatomy, and access. Upper front teeth are the most accessible; upper and lower molars with multiple roots are more complex and time-consuming.
Q2: What is recovery like after apicoectomy?
Swelling peaks at 24–48 hours and typically resolves by day 4–5. NSAIDs manage post-operative discomfort adequately for most patients. Soft diet for 7–10 days; avoid pressure on the surgical area during brushing for the first week. Most patients return to normal activities the following day.
Q3: Is there a risk of damaging adjacent teeth during the procedure?
The root apices of adjacent teeth are separated by bone and typically well clear of the surgical osteotomy. CBCT planning confirms the spatial relationship before surgery so the osteotomy can be positioned to avoid adjacent structures. Damage to adjacent teeth in a well-planned apicoectomy is uncommon.
Q4: If the apicoectomy is unsuccessful, is the tooth lost?
Not necessarily immediately. If periapical healing does not occur after apicoectomy, the options are: a second apicoectomy (less commonly indicated); intentional replantation (extraction, retrograde root treatment outside the mouth, immediate reimplantation); or extraction and implant replacement. The decision depends on the tooth’s remaining structural integrity and the patient’s priorities.