.webp)
Most patients who need full mouth rehabilitation have already spent years fixing teeth individually. A crown here, a root canal there, a bridge that eventually failed. By the time they arrive at a comprehensive consultation, many have spent more cumulatively than the rehabilitation itself would cost — without achieving a stable, predictable result.
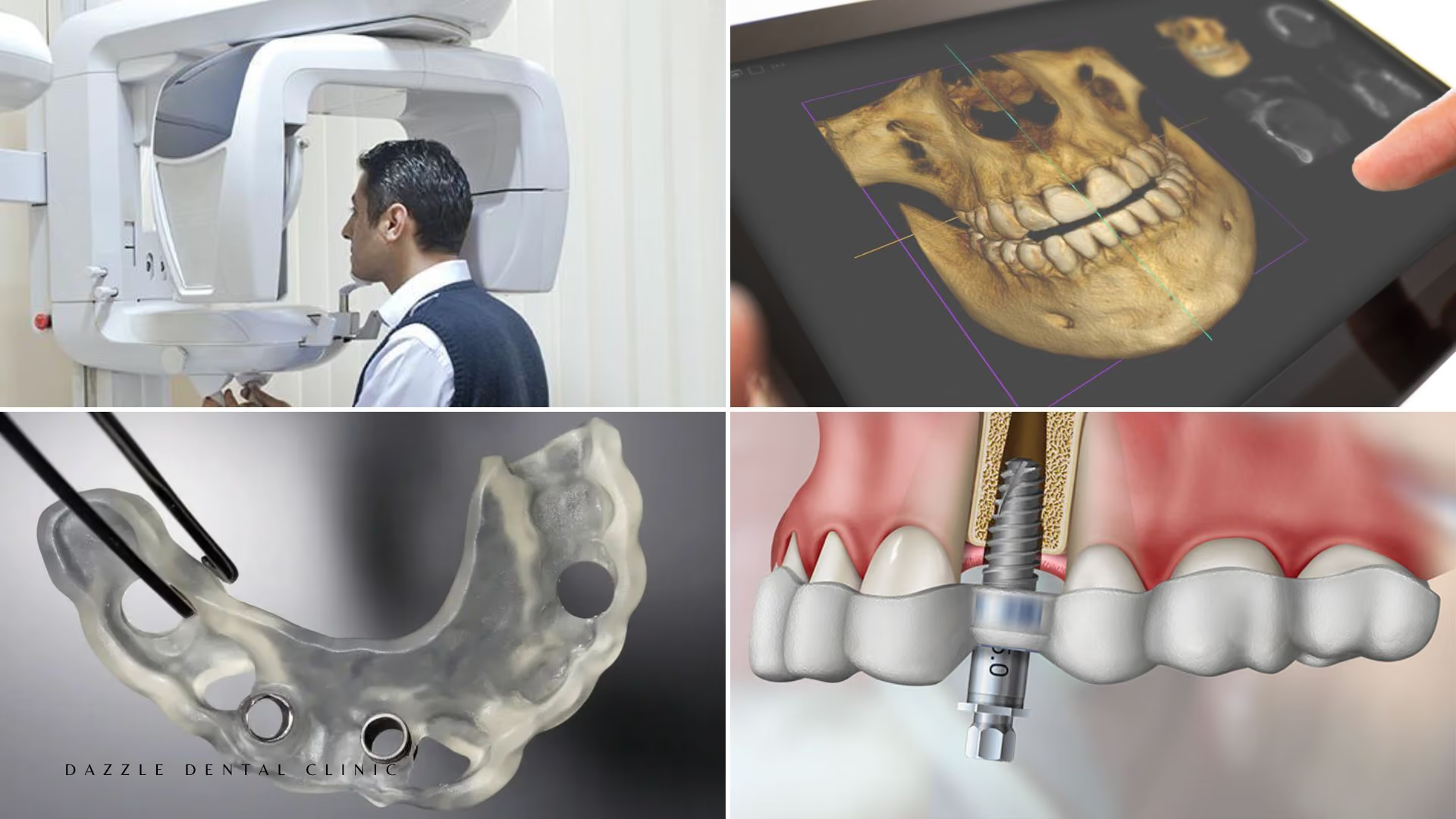
The investment argument for full mouth rehabilitation isn't about spending more. It's about spending once, correctly, on a treatment plan designed to last — rather than continuing to spend incrementally on a mouth that keeps breaking down. Full mouth rehabilitation at Dazzle routinely incorporates dental implants and where appropriate, full-arch All-on-4 rehabilitation.
What Makes Full Mouth Rehabilitation Different from Single-Tooth Treatment
Single-tooth dentistry treats problems as they present. A tooth needs a crown, it gets a crown. A tooth becomes infected, it gets a root canal. The issue is that teeth do not exist in isolation. They function as an integrated system governed by the bite, jaw position, muscle balance, and the health of supporting bone and gum tissue. When the bite is off — because of tooth loss, wear, or uncoordinated previous treatment — every tooth in the arch shares that dysfunction.
Full mouth rehabilitation addresses the system, not just the parts. Occlusion is redesigned from a stable, measured baseline. Restorations are sequenced so each one works within the whole, not against it. The result is a set of teeth that distributes bite force evenly, maintains jaw joint health, and is unlikely to generate the cascade of individual failures that defines poorly managed dental deterioration.
The Elements That Determine Whether It Lasts
Occlusal planning is where most failed rehabilitations begin to go wrong. A beautiful set of restorations placed on a bite that concentrates force on specific teeth will fracture those teeth. The bite must be evaluated, designed, and tested — using provisional restorations over weeks or months — before final restorations are placed. This is not optional. It is the step that determines whether the case holds up for 20 years or 5.
TMJ assessment matters because some patients present with rehabilitation needs that are secondary to jaw joint dysfunction. Placing restorations without addressing an underlying TMJ problem produces patients who develop chronic jaw pain after treatment, grind through their new restorations, and blame the dentist. At Dazzle, TMJ assessment is part of every full mouth rehabilitation workup.
Material selection affects longevity in ways patients don't always appreciate. E.max ceramic and zirconia have fundamentally different mechanical properties. Composite bonding, while clinically appropriate in certain cases, requires different maintenance protocols than ceramic. Applying the right material to the right tooth — based on position, bite load, and aesthetic demand — is a clinical decision, not a product choice.
Sequence and staging ensure that each phase of the rehabilitation creates a stable foundation for the next. Disease control first: active decay and periodontal disease are resolved before any restorations are placed. Structural restoration second: implants, extractions, and foundation work. Occlusal rehabilitation third: bite designed and tested provisionally. Aesthetic refinement last: the finishing layer applied once everything below it is stable.
Why Provider Expertise Is the Primary Variable
Full mouth rehabilitation is probably the most technically demanding work in dentistry. At Dazzle Dental Clinic, our rehabilitation team includes specialists in implantology, prosthodontics, periodontics, and oral surgery — working on the same case, in the same building. Our 100% digital workflow means that diagnosis, planning, provisional fabrication, and final restoration are all interconnected. And our in-house digital laboratory means every restoration is fabricated under direct clinical oversight.
The Cost of Not Acting
Patients who delay full mouth rehabilitation typically do so for one of two reasons: the cost feels prohibitive, or the situation doesn't feel urgent enough yet. The second reason is the more dangerous one. Severely deteriorated dentitions rarely stabilise spontaneously. Bone loss around compromised teeth progresses. The complexity and cost of rehabilitation increases with delay, not decreases.
FAQs
Q1: How is full mouth rehabilitation costed at Dazzle?
We provide a fully itemised treatment plan at consultation, broken down by procedure, materials, and phase. You know the total before any treatment begins. Financing options are available for patients who need to spread the investment.
Q2: What happens if I can't afford the full rehabilitation at once?
Treatment can be staged. We prioritise procedures by clinical urgency — addressing the most compromised teeth first and planning the remainder in phases that fit the patient's financial reality.
Q3: Can international patients complete full mouth rehabilitation in one trip?
Some cases can be completed or substantially advanced in a single extended visit of 2–3 weeks. Cases involving implants with osseointegration periods require at minimum two visits. We plan this specifically with international patients to make the most of each visit and minimise the number of trips required.
Q4: How long does full mouth rehabilitation last?
When properly planned and executed, 20+ years is a realistic expectation for implant-based rehabilitations. The restorations may need adjustment or selective replacement at the 15–20 year mark, but the foundation — the implants, the bone, the bite design — should be intact.