.webp)
PRF — platelet-rich fibrin — is used in implant dentistry because it accelerates the biological processes that determine how quickly and reliably healing occurs. Understanding what PRF actually does — not just that it “improves healing” — helps patients evaluate whether it is appropriate for their case and ask the right questions.
At Dazzle, PRF is incorporated into implant surgery, bone grafting, and periodontal regenerative procedures where clinical evidence supports its use. See our illustrated PRF guide for annotated case examples.
What PRF Is
PRF is an autologous biomaterial: it is made from the patient's own blood, drawn immediately before the procedure. The blood is centrifuged to separate its components. The middle layer contains a fibrin clot rich in platelets, leukocytes (white blood cells), and the growth factors these cells release. This layer — the PRF membrane or plug — is placed at the surgical site.
The Growth Factors and What They Do
Platelets release growth factors from their alpha granules when they activate. The key factors concentrated in PRF: PDGF (platelet-derived growth factor) — stimulates cell proliferation and migration; TGF-β (transforming growth factor) — regulates matrix deposition and inhibits excessive inflammatory response; VEGF (vascular endothelial growth factor) — promotes angiogenesis (new blood vessel formation), which is critical for graft vascularisation; IGF (insulin-like growth factor) — supports bone cell proliferation.
The fibrin matrix delivers these factors in a slow, sustained release as the fibrin dissolves during healing — this is more physiologically effective than a bolus delivery of growth factors, which is why injectable PRP performs differently from PRF membranes.
Applications in Implant Dentistry at Dazzle
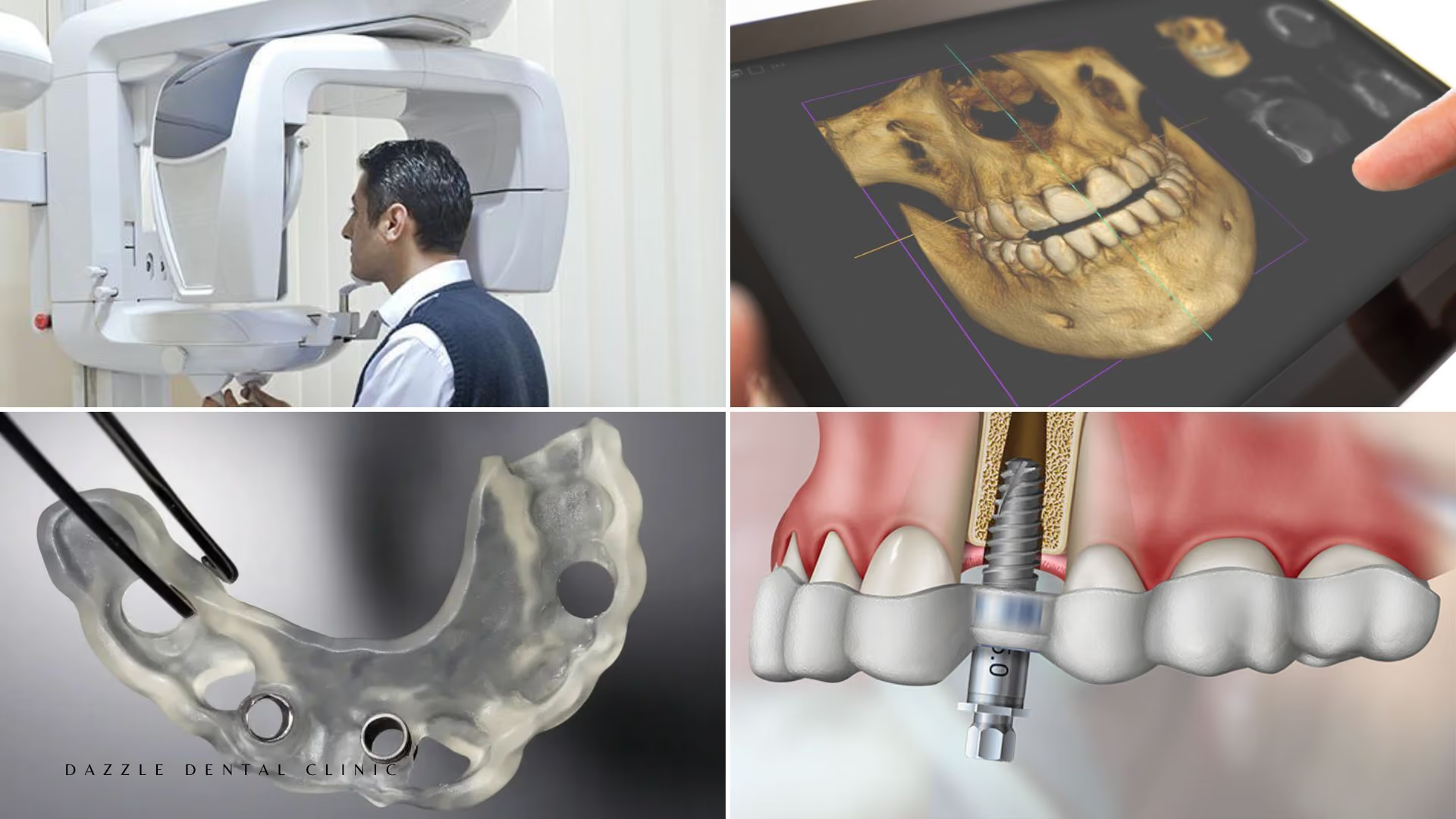
Bone grafting and sinus lifts: PRF mixed with xenograft bone material provides growth factor support at the graft matrix. The fibrin scaffold binds the graft particles and stabilises the graft volume during early healing. Published comparisons show PRF + graft vs graft alone: earlier radiographic bone density in the graft, shorter consolidation time before implant placement. For the specific sinus lift application, see our osseointegration guide.
Implant placement sites: PRF membrane placed at the implant neck and peri-implant space. Reduces early soft tissue inflammation, supports fibrin-mediated clot stability in the first week of healing, and promotes earlier epithelial coverage of the implant shoulder.
Extraction socket management: PRF plug placed at extraction. Reduces dry socket incidence, accelerates soft tissue closure, and supports socket preservation outcomes when bone graft is placed simultaneously.
What PRF Does Not Change
PRF does not change the fundamental biology of osseointegration or bone regeneration. The structural scaffold — the bone graft — still determines whether adequate bone volume is achieved. Osseointegration still requires 8–12 weeks. Sinus lifts still require 4–6 months of consolidation. PRF can shorten these timelines modestly and improve outcome quality, but it is an adjunct to correctly planned surgery, not a substitute for it.
FAQs
Q1: Does PRF hurt? Is blood drawing required on the day of surgery?
Yes — a small blood sample is drawn at the clinic immediately before the procedure. This is a straightforward venepuncture, similar to a routine blood test. Processing takes 10–15 minutes and occurs while other pre-surgical preparations are being made.
Q2: Is PRF safe for patients with blood conditions?
PRF is derived from the patient's own blood, so there is no external biological material risk. Patients with clotting disorders or on anticoagulants may have altered platelet function that affects PRF quality — this is assessed at the pre-surgical medical history review.
Q3: Will I recover faster because of PRF?
In some measurable respects: yes. Soft tissue closure over the implant site occurs earlier with PRF. Patients with PRF in extraction sockets report less dry socket and faster closure. The day-to-day subjective recovery experience — swelling and discomfort — is modestly improved in most published comparisons but not dramatically different.
Q4: Is PRF included in the implant cost at Dazzle?
At Dazzle, PRF preparation is included in implant surgery and bone grafting procedures where it is used. It is not charged as a separate add-on item.