.webp)
Endodontic retreatment — a second root canal procedure on a tooth that has already been treated — is necessary when the original treatment fails to fully eliminate infection, or when reinfection occurs after treatment. It is a more demanding procedure than the original root canal because the first step requires removing all the previously placed filling material before the canals can be reassessed and re-treated. Understanding why root canals fail, and what retreatment involves, helps patients make decisions about whether to pursue it or consider extraction.
Why Root Canal Treatment Fails
Missed canals: The most frequent cause. Human teeth have more canals than their basic descriptions suggest — maxillary first molars routinely have 3–4 canals, occasionally 5; mandibular premolars can have two canals in a single root. If a canal is missed at the original treatment, it remains infected and will eventually cause periapical pathology. Under a microscope, missed canals are identifiable and treatable. Without magnification, they are invisible.
Incomplete obturation: The root filling does not reach the apex of the canal or leaves voids. Bacteria survive in the unfilled space and sustain the periapical infection. This is visible on radiographs as a short fill or radiolucent gap.
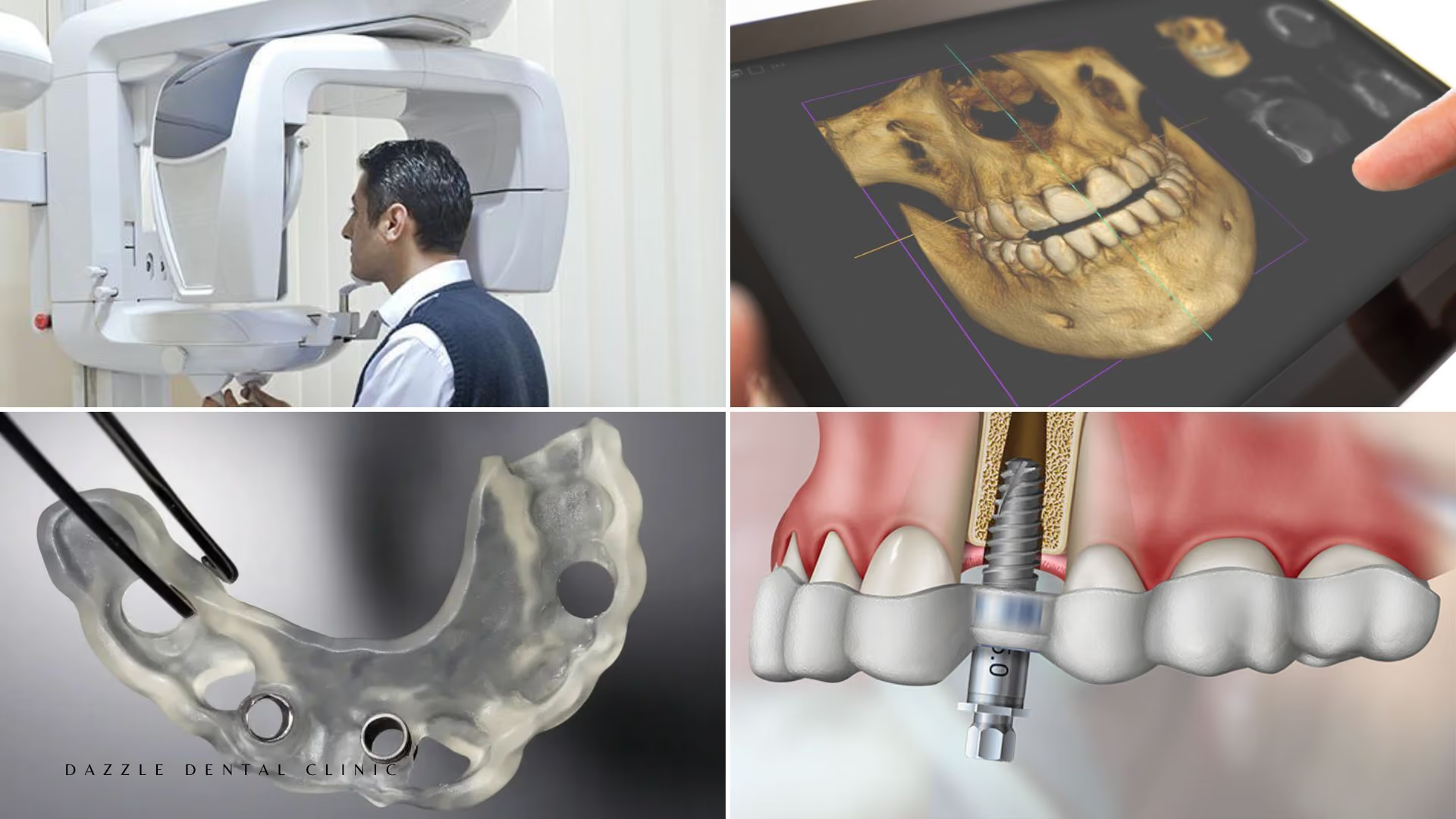
Complex anatomy: Canal curves, fins, isthmuses, and C-shaped canal configurations create spaces that standard rotary instruments cannot fully clean. Bacteria persist in these anatomical recesses. CBCT imaging before retreatment provides a three-dimensional map of the canal anatomy — see our CBCT scanning guide for how this information changes treatment planning.
Coronal microleakage: The most preventable cause. When a root canal-treated tooth is not restored promptly with an adequate coronal seal (ideally a crown), bacteria from the oral environment re-enter the canal system through the restoration. A technically perfect root canal fails if the coronal restoration fails.
Vertical root fracture: A crack extending vertically through the root allows bacteria persistent access regardless of retreatment. Vertical fractures are a contraindication to retreatment — the tooth cannot be saved by endodontic means.
What Retreatment Involves
Retreatment begins with removal of the previous crown or access restoration to re-enter the tooth. The existing gutta-percha filling (the pink/orange rubbery material that seals root canals) must be removed. This is done using a combination of heat-softening, solvents (typically chloroform or eucalyptol), and hand files under the operating microscope. Complete removal of the previous fill is essential — residual gutta-percha at the apex masks and harbours bacteria.
Once the canals are cleared, the procedure follows the same sequence as initial treatment but with additional scrutiny for missed anatomy: the entire canal system is explored under microscope magnification (typically 8–16x), and transillumination of the pulp floor helps identify missed canal orifices. CBCT imaging before retreatment provides a three-dimensional map of the canal anatomy — at Dazzle, CBCT is used for complex retreatment cases where the original radiograph suggests unusual anatomy or when the periapical lesion has not resolved after initial treatment.
Canals are re-instrumented with rotary nickel-titanium files to shape the canal to its working length. Irrigation with sodium hypochlorite (NaOCl) and EDTA removes the smear layer and disinfects the canal walls. Ultrasonic activation of the irrigant improves penetration into lateral canals and isthmi that rotary instrumentation cannot reach. Once the canals are clean, dry, and confirmed bacteria-free (or as close as possible), they are re-obturated with warm vertical condensation gutta-percha and sealed at the orifice level.
Success Rates for Retreatment
Published success rates for endodontic retreatment: 70–85% periapical healing at 2–4 years in cases where the original failure was due to coronal leakage, incomplete obturation, or missed canals. Success rates are lower when the original failure was due to persistent infection with resistant organisms (e.g., Enterococcus faecalis biofilm) or complex untreatable anatomy.
Retreatment success is significantly higher when performed under the operating microscope — the microscope is what allows previously missed canals to be found and allows more complete removal of previous filling material. At Dazzle, retreatment is performed under microscope magnification as standard, not as a premium option.
When Retreatment Is Not Appropriate
Retreatment is not indicated when: a vertical root fracture is present (the tooth requires extraction); the periodontal prognosis of the tooth is poor regardless of endodontic outcome (bone loss making the tooth structurally unviable); or when the strategic value of the tooth in the overall treatment plan does not justify the complexity and cost of retreatment versus implant replacement. At Dazzle, these decisions are made within a multidisciplinary assessment, not solely by the endodontist.
FAQs
Q1: Is retreatment more painful than the original root canal?
Under local anaesthesia, neither procedure is painful during treatment. Post-retreatment soreness is typically similar to or slightly more than the original treatment because the canal has more manipulation time and the periapical tissues may be more inflamed. NSAIDs manage this effectively for most patients over 3–5 days.
Q2: How many appointments does retreatment take?
Most retreatment cases at Dazzle are completed in 1–2 appointments. Appointment 1: removal of existing fill, canal exploration, and preparation. If the canals cannot be fully disinfected in one session, a calcium hydroxide dressing is placed and the tooth is temporised for 2–4 weeks. Appointment 2: completion of obturation and referral for crown.
Q3: What if retreatment doesn’t work?
If retreatment fails to resolve the periapical pathology, apicoectomy (surgical endodontics — removal of the root tip and retrograde seal through a small gum incision) is the next option before considering extraction and implant replacement. Apicoectomy has published success rates of 85–90% at 2 years in appropriate cases.
Q4: Why does a root canal-treated tooth need a crown so quickly after retreatment?
The endodontic treatment seals the root canal system. It does not restore the structural integrity of the crown. A devitalised posterior tooth without a crown is at high risk of cusp fracture — and a cusp fracture below the gumline in a root canal-treated tooth often makes the tooth unrestorable. The window between retreatment completion and crown placement should be weeks, not months.