














.webp)
Every regenerative periodontal procedure — whether GTR with a membrane, bone grafting, or PRF application — depends on the quality of the root surface at the site of treatment. A membrane placed over a contaminated root creates a regenerative environment on top of a failed foundation.
Root surface preparation is not simply cleaning. It is the systematic elimination of bacterial biofilm, calculus, endotoxin-contaminated cementum, and bacterial toxins that have penetrated the root surface during periodontal disease — combined, where appropriate, with conditioning to enhance the biological compatibility of the surface for new tissue attachment.
What Root Surface Contamination Looks Like
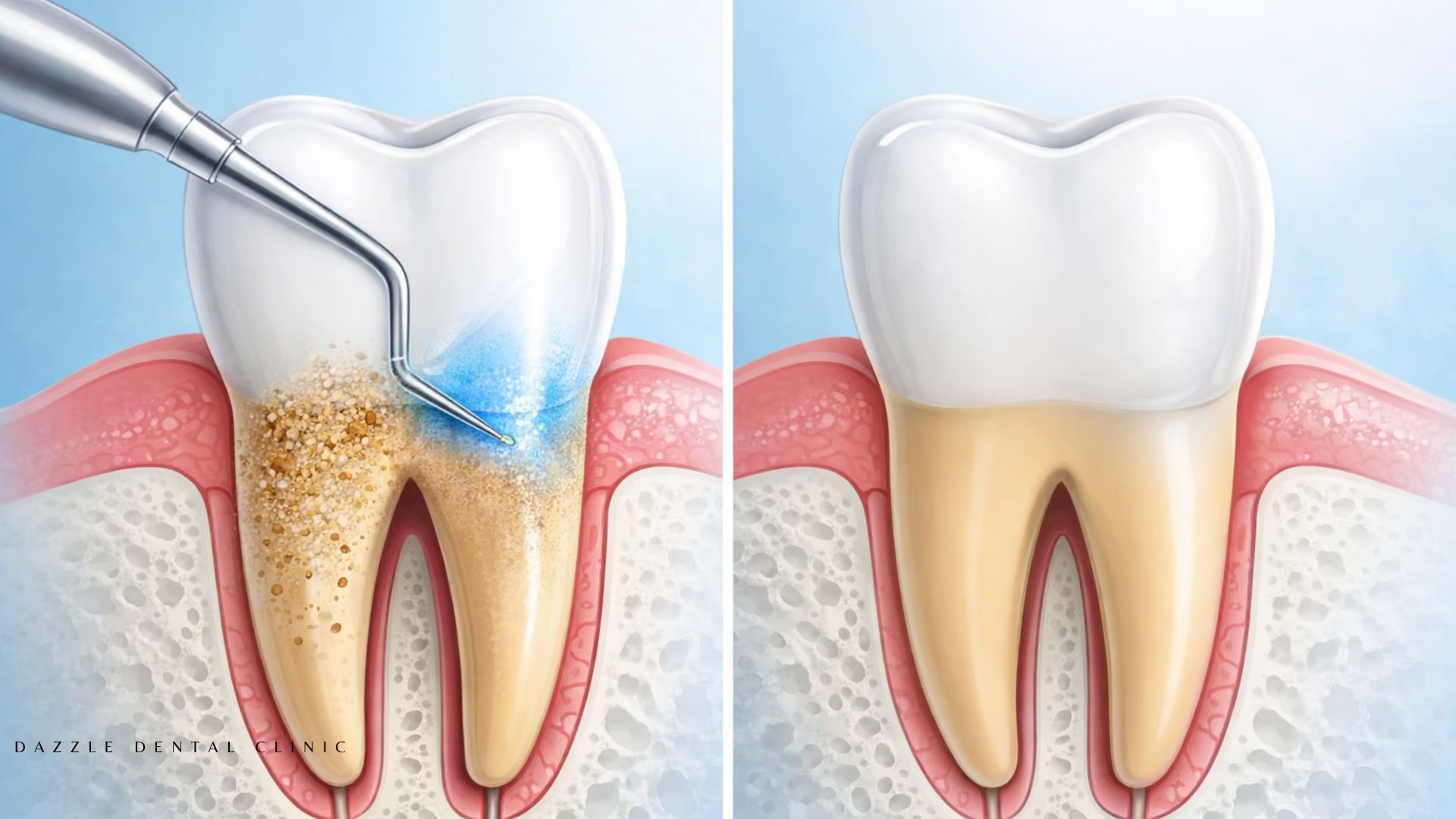
In periodontal disease, bacteria in the deepened gingival pocket attach to the root surface and mineralise into calculus. Bacterial endotoxins penetrate superficially into the cementum. If this contaminated cementum remains at the time of regenerative surgery, it prevents the key cells (periodontal ligament fibroblasts, osteoblasts) from attaching to the root and forming new attachment. The goal of root surface preparation is to remove all calculus and endotoxin-contaminated cementum, leaving a clean surface the regenerating cells can populate. For details on how these regenerative cells work, see our periodontal attachment regeneration guide.
Instruments and Techniques
Ultrasonic scalers: High-frequency vibration combined with water irrigation removes calculus and biofilm efficiently across root surfaces, including concavities and furcation areas that hand instruments struggle to reach.
Hand curettes: Gracey curettes — area-specific instruments designed for each surface of each tooth — allow tactile feedback during root planing that ultrasonic instruments cannot provide. The clinician feels the transition from calculus to clean root surface. In surgical access cases (where the flap is elevated), hand curettes allow direct visual and tactile confirmation of complete calculus removal.
Laser-assisted debridement: Erbium and Nd:YAG lasers are used at Dazzle as adjuncts in specific cases for bacterial decontamination of root surfaces and the surrounding pocket tissue.
Root Surface Conditioning for Regenerative Procedures
Before placing regenerative materials (membrane, graft, PRF) in GTR procedures, the prepared root surface may be chemically conditioned with citric acid or EDTA. EDTA conditioning removes the smear layer left by instrumentation, exposing collagen fibres in the root surface that provide a scaffold for PDL fibroblast attachment and fibrin clot formation from the PRF membrane. For the specific PRF protocols used in periodontal regeneration at Dazzle, see our PRF in dentistry guide.
Non-Surgical vs. Surgical Root Surface Preparation
Non-surgical root surface preparation is the first-line treatment for most periodontal disease, effective for pockets up to 5–6mm. For deeper pockets (7mm+), furcation involvement, or sites scheduled for GTR, surgical access provides direct visual confirmation of complete debridement. This is the setting where root conditioning is typically applied before membrane placement.
FAQs
Q1: Is root surface preparation the same as scaling and cleaning?
Scaling removes tartar from above and just below the gumline. Root surface preparation involves systematic debridement of the entire root surface within the periodontal pocket, extending to the base of the defect. It is more thorough and typically requires local anaesthesia. Routine scaling does not achieve the level of root surface decontamination needed before regenerative procedures.
Q2: How many appointments does root surface preparation take?
For non-surgical full-mouth root planing, treatment is typically divided into two or four appointments treating quadrants separately. For surgical GTR cases, root surface preparation is part of the surgical procedure itself.
Q3: Does root surface preparation hurt?
Under local anaesthesia, the procedure is comfortable. Post-procedure sensitivity is expected for 1–4 weeks and is managed with desensitising agents and over-the-counter analgesics.
Q4: How do I know if my root surface preparation was thorough?
Clinically, the response at 6–8 weeks is the best indicator. Pocket depth reduction, reduction in bleeding on probing, and improved tissue tone are all signs of effective root surface preparation. Residual pockets that don't respond to non-surgical treatment are candidates for surgical access and definitive root surface treatment under direct vision.

.avif)






