.webp)
Accurate diagnosis is the precondition for accurate treatment. At Dazzle Dental Clinic, three imaging modalities form the diagnostic backbone of clinical decision-making: CBCT 3D scans, digital periapical and bitewing X-rays, and OPG (orthopantomogram) panoramic imaging. Each captures different information and serves different clinical purposes. Using the right imaging tool for the right question is as important as having the technology available.
OPG: The Overview Tool
An OPG (orthopantomogram) is a panoramic radiograph that produces a single wide-field image covering the entire dentition, both jaws, the temporomandibular joints, and the maxillary sinuses. It is the appropriate starting point for a new patient assessment, orthodontic evaluation, wisdom tooth assessment, and surgical planning where a whole-arch overview is needed before committing to higher-detail imaging.
What OPG shows well: gross bone levels across the full arch, relative positions of tooth roots and impacted teeth, obvious pathology (cysts, large periapical lesions, gross bone loss), jaw joint anatomy, and the relationship of third molar roots to the inferior alveolar nerve canal (though 2D projection means this relationship cannot be measured in the depth dimension without CBCT).
What OPG cannot show: bone width (the buccal-palatal dimension), precise bone height measurements at individual sites, or small periapical lesions obscured by root superimposition. It is a screening tool, not a measurement tool.
Digital Periapical and Bitewing X-Rays: Tooth-Level Detail
Digital periapical films provide higher resolution than OPG for individual teeth — sufficient to detect caries between teeth, assess root morphology, evaluate the quality and length of endodontic treatment, and monitor periapical lesion healing at 6-monthly intervals. Bitewing films are specifically optimised for detecting interproximal (between-teeth) caries in the posterior dentition, showing the crowns of upper and lower teeth simultaneously.
Digital X-rays at Dazzle deliver approximately 80% less radiation than conventional film radiographs. The image is available immediately on screen — no darkroom development. Digital brightness and contrast adjustments enhance diagnostic detail without additional exposure. Radiation dose for a full-mouth periapical series: approximately 35–80 microsieverts — comparable to 2–3 hours of natural background radiation.
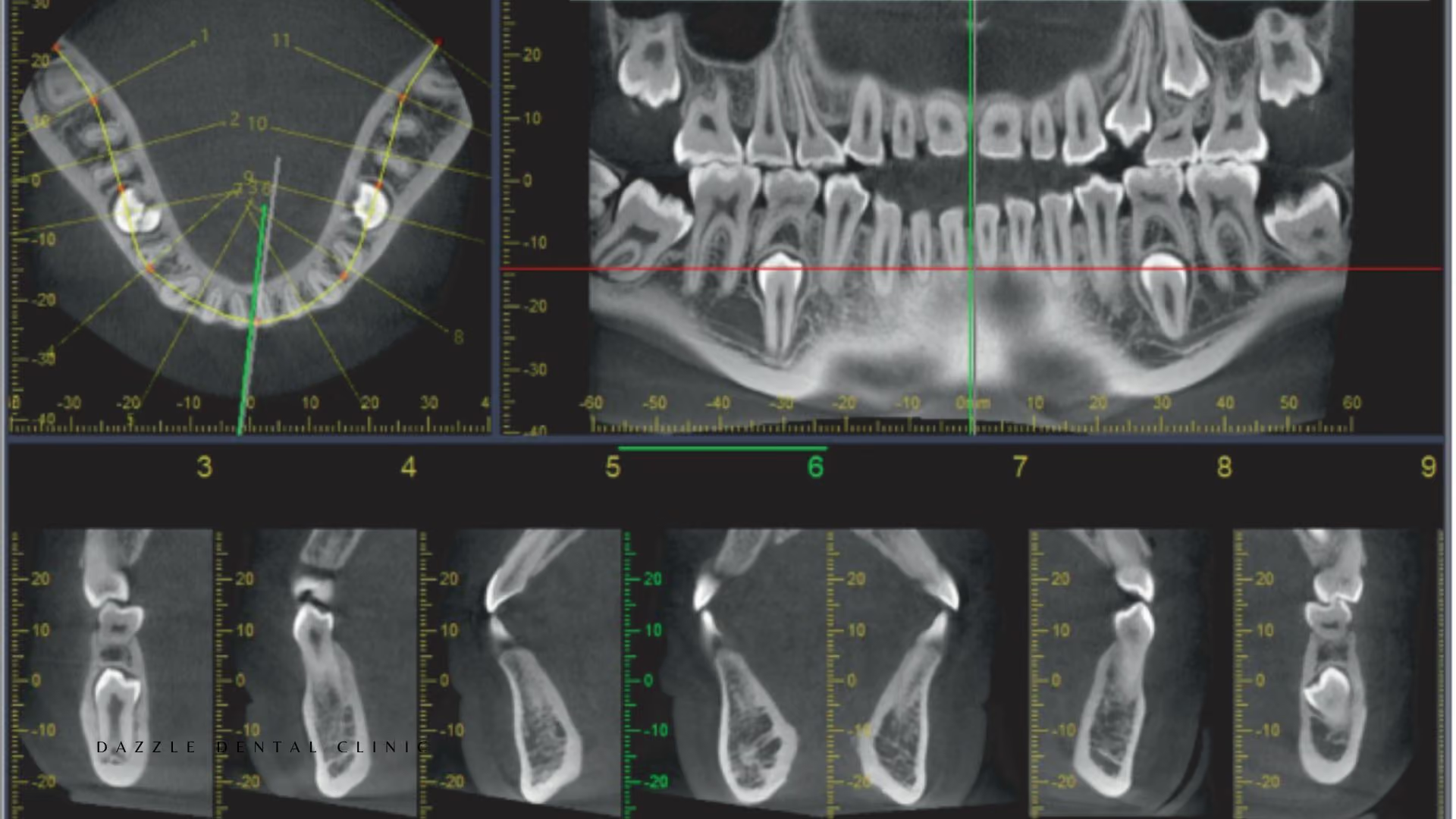
CBCT: Three-Dimensional Volumetric Imaging
CBCT captures a volumetric dataset from which images are reconstructed in any plane — axial, coronal, sagittal, and panoramic. The critical clinical advantage is the third dimension: bone height, width, and density are all measurable at any specific site, and anatomical structures can be located precisely in three dimensions rather than inferred from two-dimensional projections. For full detail on how CBCT is used for implant planning, see our dedicated CBCT guide.
At Dazzle, CBCT is indicated for: all full-arch implant planning (All-on-4, All-on-6, zygomatic); single implant cases where bone volume is uncertain; zygomatic and pterygoid implant trajectory planning; complex endodontic retreatment cases; third molar extraction where the panoramic suggests nerve proximity; and sinus lift planning.
CBCT is not used as a routine screening tool — the ALARA (as low as reasonably achievable) principle applies. A CBCT is ordered when the information it provides is expected to change the clinical decision. Effective dose for a small field-of-view dental CBCT: 20–100 microsieverts, comparable to a full-mouth periapical series.
Using All Three Together
For a complex implant case at Dazzle, the typical imaging sequence is: OPG on initial assessment (overview, screening for obvious pathology); CBCT for surgical planning (bone measurements, nerve mapping, sinus assessment); digital periapicals at placement, 3-month review, and annual maintenance (marginal bone level monitoring at each implant). Each modality contributes information the others cannot provide. This feeds directly into the digital guided surgery workflow.
FAQs
Q1: Do I need a CBCT before a single dental implant?
Not always. For posterior implants where a periapical film and clinical measurement suggest adequate bone, CBCT may not change the clinical decision. For anterior implants where the buccal bone thickness is critical, for sites with previous pathology, or where the panoramic raises any uncertainty about the inferior alveolar nerve or sinus floor proximity, CBCT is indicated. At Dazzle, this is assessed case by case.
Q2: How often should dental X-rays be taken?
Bitewing radiographs for caries detection: every 12–24 months in low-risk adults, more frequently in high-risk patients. Periapical films of implants: at placement, 3 months, 6 months, then annually. Full-mouth periapical series: as clinically indicated, not on a fixed schedule. OPG: when a whole-arch overview is needed, typically at new patient assessment and before complex treatment.
Q3: Can I use a CBCT I had done elsewhere for treatment planning at Dazzle?
Yes. Send the DICOM files (full volumetric dataset, not PDF or screen captures) for import into our planning software. Scans older than 6–12 months may not reflect current bone levels at post-extraction sites. International patients routinely send DICOM files for remote pre-treatment assessment before travelling.
Q4: What is the radiation dose of a CBCT compared to a medical CT?
A small field-of-view dental CBCT delivers approximately 20–100 microsieverts. A medical CT of the head delivers approximately 2,000 microsieverts. A chest CT delivers approximately 7,000 microsieverts. The dental CBCT dose is substantially lower than medical CT because the cone beam geometry and smaller detector area expose a much smaller tissue volume.
.avif)