














.webp)
CBCT (Cone Beam Computed Tomography) and conventional two-dimensional radiography — panoramic OPG, periapical films, bitewings — produce fundamentally different information. Understanding the difference helps patients understand why their clinician is recommending a CBCT scan and what it is expected to change about their treatment.
What Conventional 2D Radiography Shows
A panoramic OPG (orthopantomogram) provides a flattened overview of the entire dentition, both jaws, the temporomandibular joints, and the upper sinuses in a single image. It shows gross bone levels, tooth positions, large pathology, and the general relationship between structures. Periapical films provide higher-resolution views of individual teeth — better for detecting periapical lesions, root morphology, and the quality of endodontic treatment.
The limitation of all 2D radiographs is dimensional collapse: a three-dimensional structure is projected onto a two-dimensional film, so the depth dimension is lost. Two structures overlying each other in the beam’s path appear superimposed. The buccal (outer) bone plate, which is the first to resorb in periodontal disease or after extraction and the most important dimension for implant planning, is not measurable from a 2D radiograph.
What CBCT Adds
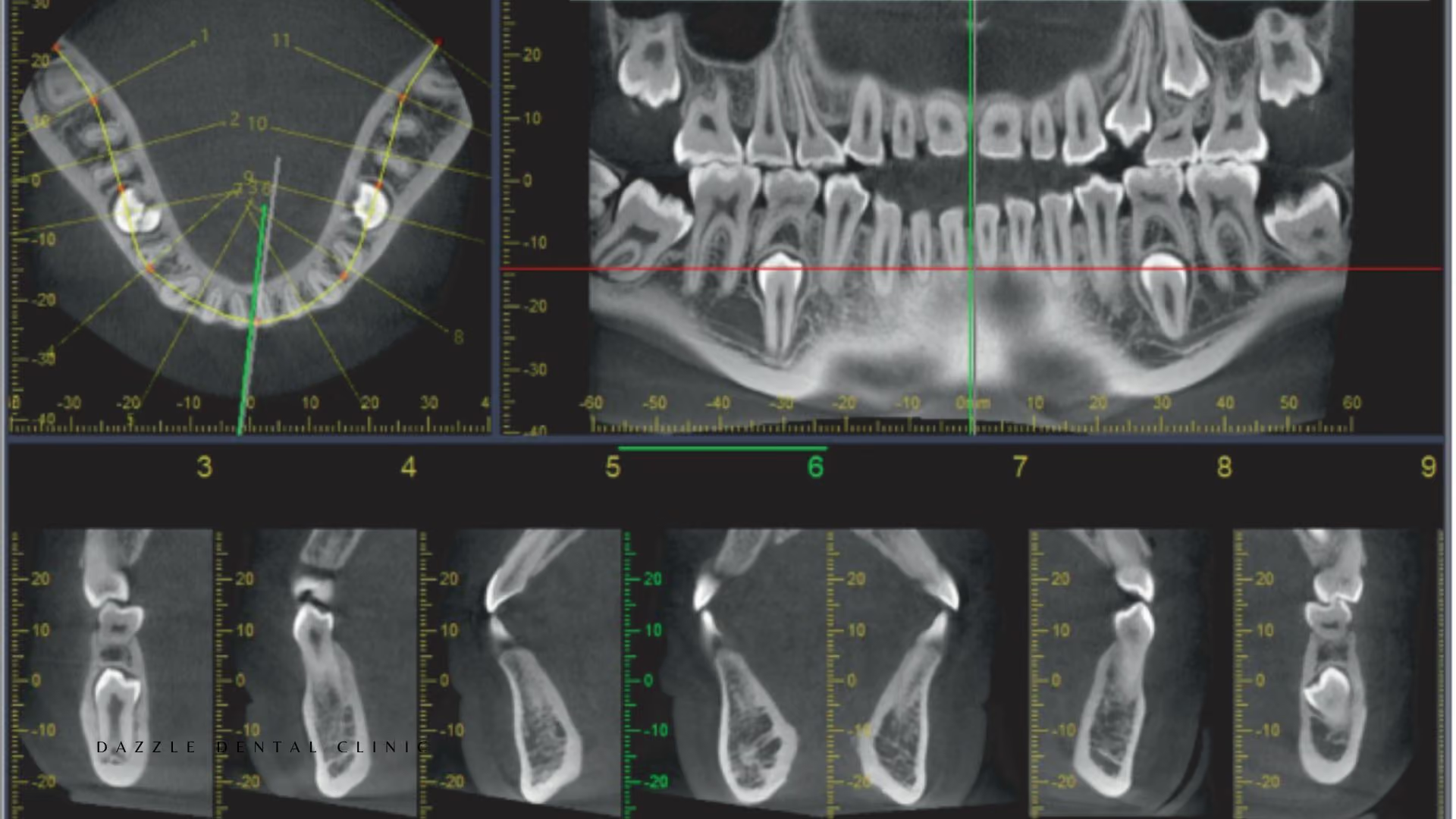
CBCT captures a volumetric dataset of the scanned area from which images can be reconstructed in any plane: axial (horizontal), coronal (front-to-back), and sagittal (side-to-side) cross-sections; panoramic reconstruction equivalent to an OPG; and three-dimensional surface renders. The critical addition over 2D is the ability to measure bone in three dimensions — height, width, and density — at any specific location.
For implant planning: CBCT shows the bone height from the crest to the sinus floor at each posterior upper jaw site, the bone width available for the implant diameter, the course of the inferior alveolar nerve in the lower jaw, and the density of the bone (which correlates with the Misch classification and determines what primary stability is achievable). None of these measurements are available from a panoramic.
For endodontics: CBCT shows the three-dimensional anatomy of the root canal system — accessory canals, C-shaped configurations, root curvature angles, and the location of periapical lesions relative to adjacent anatomy. A small periapical lesion between two roots can be missed on a periapical film if the adjacent roots are superimposed; CBCT shows it clearly.
For surgical planning: CBCT shows the precise position of the inferior alveolar nerve relative to impacted wisdom tooth roots, the relationship of pathology to adjacent structures, and the sinus anatomy for sinus lift procedures.
Radiation Dose Comparison
CBCT delivers a lower radiation dose than a medical CT scan because the cone beam geometry and smaller detector area expose less tissue than the fan beam geometry of medical CT. Typical effective dose: a small field-of-view dental CBCT is approximately 20–100 microsieverts (μSv); a full-mouth periapical series (18 films) is approximately 35–80 μSv; a panoramic OPG is approximately 15–20 μSv; a medical chest CT is approximately 7,000 μSv. The radiation dose of a dental CBCT is comparable to a few days of background radiation exposure.
CBCT is not appropriate for every patient — the “as low as reasonably achievable” (ALARA) principle applies, and a CBCT is justified only when it provides information that will change treatment planning. At Dazzle, CBCT is recommended when the information it provides is expected to meaningfully change the treatment plan; it is not used as a routine screening tool.
When CBCT Changes the Clinical Decision
Implant placement planning: always, for full-arch cases; for single implants where bone volume adequacy is uncertain from clinical examination. Zygomatic and pterygoid implant planning: always — the zygomatic trajectory and pterygoid plate anatomy require three-dimensional assessment. Endodontic retreatment of complex cases: when standard radiographs suggest unusual anatomy or when a previous root canal has failed and the reason is not apparent from 2D imaging. Impacted third molar removal: when the panoramic suggests proximity of the roots to the inferior alveolar nerve canal. TMJ assessment: when the clinical history and panoramic suggest joint pathology requiring three-dimensional evaluation.
FAQs
Q1: Is a CBCT scan safe?
Yes. The radiation dose is low — comparable to a few days of background radiation at sea level. For patients who are pregnant, CBCT is deferred unless the clinical need is urgent and cannot be addressed by non-radiographic means. For all other patients, the clinical benefit of the additional information justifies the minimal dose when the scan is appropriately indicated.
Q2: How long does a CBCT scan take?
The scan itself takes 8–20 seconds of rotation time. The total time in the room, including positioning and the scan, is approximately 5 minutes. Image reconstruction and review by the implantologist or specialist takes longer and may be done before the next appointment.
Q3: Can I bring my CBCT from another clinic?
Yes. DICOM files from a CBCT performed elsewhere can be imported into Dazzle’s planning software for review. International patients sending DICOM files for remote pre-assessment should send the full DICOM dataset (not just screen captures or PDF renders), as the planning software requires the original volumetric data to take measurements. Scans older than 6–12 months may not reflect current bone volume accurately, particularly in post-extraction sites.
Q4: Will my CBCT scan be interpreted by a specialist?
At Dazzle, CBCT scans are reviewed by the treating clinician for the specific purpose for which they were ordered — implant planning, surgical assessment, endodontic evaluation. Complex or atypical findings are referred to a maxillofacial radiologist for formal interpretation report.


.avif)





