














.webp)
Dental radiography is not one technology — it is a family of modalities each suited to different clinical questions. Ordering the wrong imaging for a clinical situation either produces insufficient information (leading to planning gaps) or exposes the patient to unnecessary radiation. At Dazzle Dental Clinic, imaging is selected based on clinical indication, with each modality chosen because it answers a specific diagnostic question the other modalities cannot.
Digital Periapical Radiographs
Dose: 1–5 μSv (digital). Indication: single-tooth or single-site diagnosis. Provides: periapical bone assessment (abscess, granuloma, cyst), root length and morphology, inter-proximal bone level for periodontal staging, crown/restoration margin evaluation, post-endodontic fill assessment, implant marginal bone monitoring. Limitation: shows bone height only; cannot show bone width or three-dimensional root/bone relationships.
Taken at Dazzle with paralleling technique and film holder to ensure consistent image geometry — critical when serial images are used to monitor marginal bone levels around implants or periodontal sites over time.
Digital OPG (Orthopantomogram / Panoramic Radiograph)
Dose: 12–15 μSv (digital). Indication: full-arch overview. Provides: all teeth, both jaws, sinus floors, inferior alveolar nerve canals, condylar morphology, third molar position, and jaw lesions in a single exposure. Used for: initial comprehensive assessment of a new patient, third molar evaluation, screening before CBCT for implant planning, orthodontic root development assessment, gross jaw pathology screening.
The OPG is the appropriate initial imaging for complex cases but is insufficient as the sole modality for implant planning. It cannot show bone width at proposed implant sites, does not represent the inferior alveolar nerve’s depth below the proposed implant site accurately due to magnification variability, and produces distortion artifacts at the anterior midline. It screens for problems that CBCT then characterises.
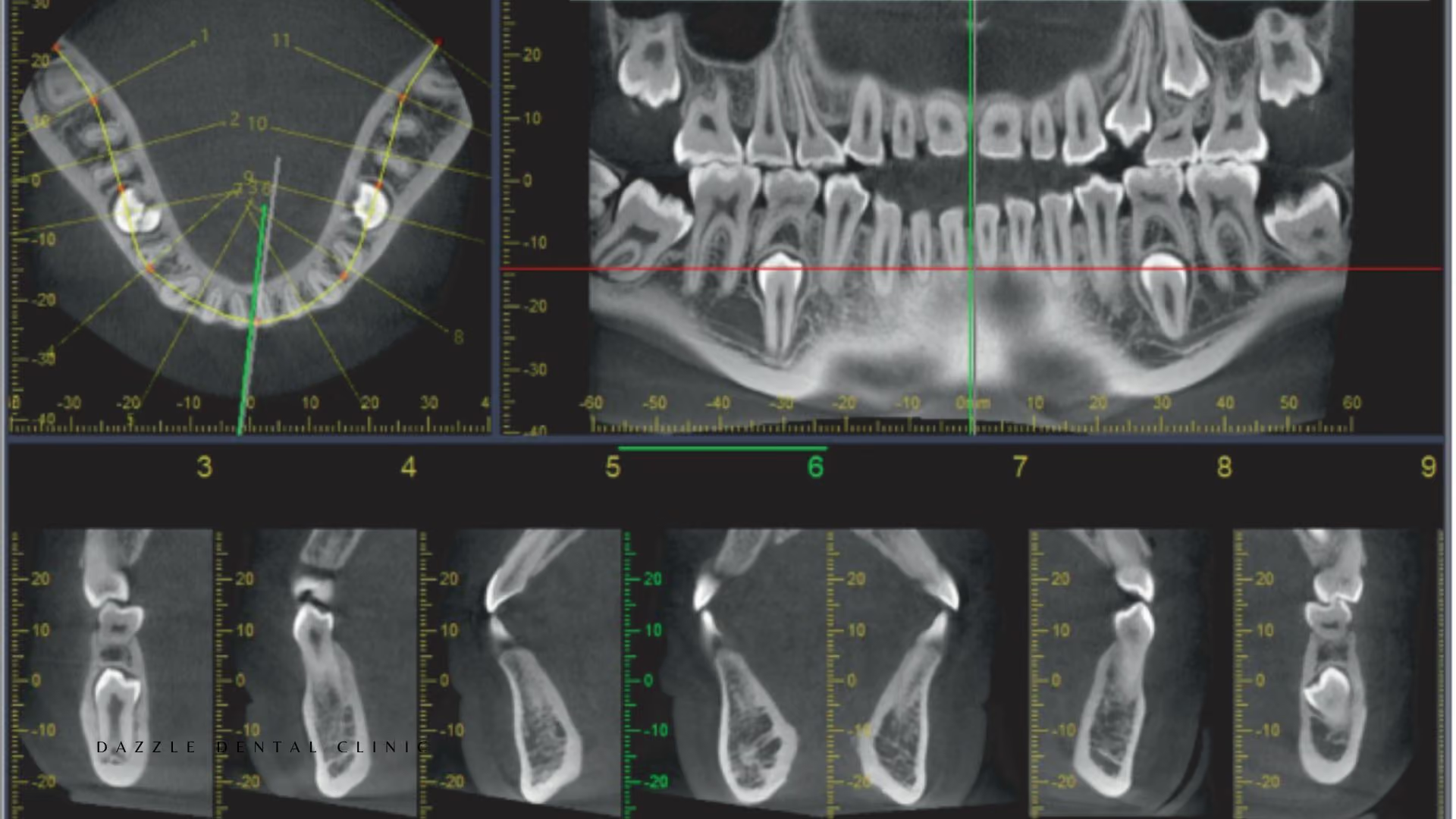
CBCT (Cone Beam Computed Tomography)
Dose: 20–40 μSv (small FOV single quadrant) to 60–100 μSv (large FOV full arch). Indication: any case requiring three-dimensional anatomical information. Provides: bone width and height at proposed implant sites; Misch Type I–IV bone density classification; precise nerve canal and sinus floor location in three dimensions; root canal anatomy (MB2 canals, root fractures, periapical lesion extent); impacted tooth position relative to adjacent roots, nerves, and sinuses; condylar morphology for TMJ assessment; defect morphology for GTR planning.
CBCT is standard for all implant cases at Dazzle (single implants included), all zygomatic and pterygoid implant assessments, complex endodontic cases, and surgical planning for bone augmentation. The CBCT data feeds the virtual surgical plan from which the 3D-printed surgical guide is produced.
Lateral Cephalometric Radiograph
Dose: 5–10 μSv. Indication: orthodontic and orthognathic assessment. Provides: skeletal relationship between upper and lower jaw (ANB angle, SNA/SNB); incisor inclinations; facial soft tissue profile; growth pattern assessment. Used for: comprehensive orthodontic treatment planning, orthognathic surgery planning, assessment of skeletal discrepancy versus dentoalveolar compensation.
Cephalometric analysis at Dazzle is used for orthodontic cases, combined orthodontic-restorative cases where jaw alignment affects the restorative outcome, and for patients being assessed for orthognathic surgery referral.
Digital Bitewing Radiographs
Dose: 1–5 μSv per image. Indication: early interproximal caries detection and periodontal bone level screening. Provides: early proximal cavities not visible clinically; crestal bone levels at all posterior teeth simultaneously; calculus visualisation subgingivally. Used at Dazzle for new patient comprehensive assessment and recall appointments where caries risk is elevated.
Combining Modalities for Complex Cases
Full-mouth rehabilitation: OPG (initial overview) + CBCT (implant sites and bone assessment) + periapical series (periodontal staging and endodontic review). Orthodontic-surgical case: OPG + lateral cephalometric + CBCT for skeletal analysis. Zygomatic implant: large FOV CBCT is non-negotiable. Endodontic retreatment: periapical (initial) + small FOV CBCT (anatomy, missed canals, fracture assessment). TMJ disorders: OPG (condylar screening) + CBCT (detailed condylar morphology).
FAQs
Q1: Can I bring imaging from another clinic?
Yes. DICOM files from CBCT scans taken within the past 6–12 months can be used for treatment planning at Dazzle. Digital OPG and periapical images are also accepted. International patients regularly provide imaging for remote assessment before travel.
Q2: Is the radiation from multiple imaging sessions in a treatment course dangerous?
No. The total dose from a full implant treatment imaging sequence at Dazzle (one CBCT + 5–8 periapical + one OPG) is approximately 100–160 μSv — equivalent to roughly one transatlantic flight of cosmic radiation exposure. This is spread over several months and does not represent a meaningful health risk.
Q3: Why is CBCT needed even for a single implant when the site looks straightforward?
Because “looks straightforward” on a 2D OPG does not mean straightforward in three dimensions. Bone width, density, the precise inferior alveolar nerve depth, and sinus floor proximity are not accurately assessable from 2D imaging. A site that appears to have adequate bone height on OPG can have a bone width of 3mm or a nerve at an unusual depth. The CBCT resolves this before surgery, not during it.
Q4: How is the imaging data used after it’s taken?
The CBCT DICOM data is imported into virtual surgical planning software where the implant is placed digitally before any surgery. This plan is used to print the surgical guide. Imaging data is stored digitally and made available on request for patients’ home dental records.

.avif)






