














.webp)
Wisdom teeth — the third molars — typically emerge between ages 17 and 25. The decision to extract should be based on specific clinical findings, not on the wisdom tooth's mere presence. Our wisdom tooth surgery service at Dazzle is performed by an oral and maxillofacial specialist, with regular dental check-ups identifying wisdom tooth problems before symptoms develop.
When Extraction Is Actually Necessary
Impaction: A wisdom tooth that cannot fully erupt because it is blocked by the adjacent second molar, the jaw bone, or insufficient space. Partial eruption creates a space called the operculum that is impossible to clean properly, leading to recurrent bacterial accumulation and infection (pericoronitis). Full impaction within bone, if asymptomatic and stable on radiographic monitoring, may not require immediate removal.
Pericoronitis: Infection of the tissue surrounding a partially erupted wisdom tooth. A single episode may be managed with antibiotics and chlorhexidine irrigation, but recurrent pericoronitis is an indication for extraction.
Caries in the wisdom tooth or the adjacent second molar: The inaccessibility of the wisdom tooth's distal surface for cleaning frequently leads to decay in that area, or in the second molar's distal surface. If the wisdom tooth is causing caries in the second molar through impaction, this is a strong indication for removal.
Periodontal disease at the second molar: Partially erupted or impacted wisdom teeth create a periodontal pocket on the distal of the adjacent second molar. For more on how periodontal disease is assessed and managed at Dazzle, see our diagnosis guide.
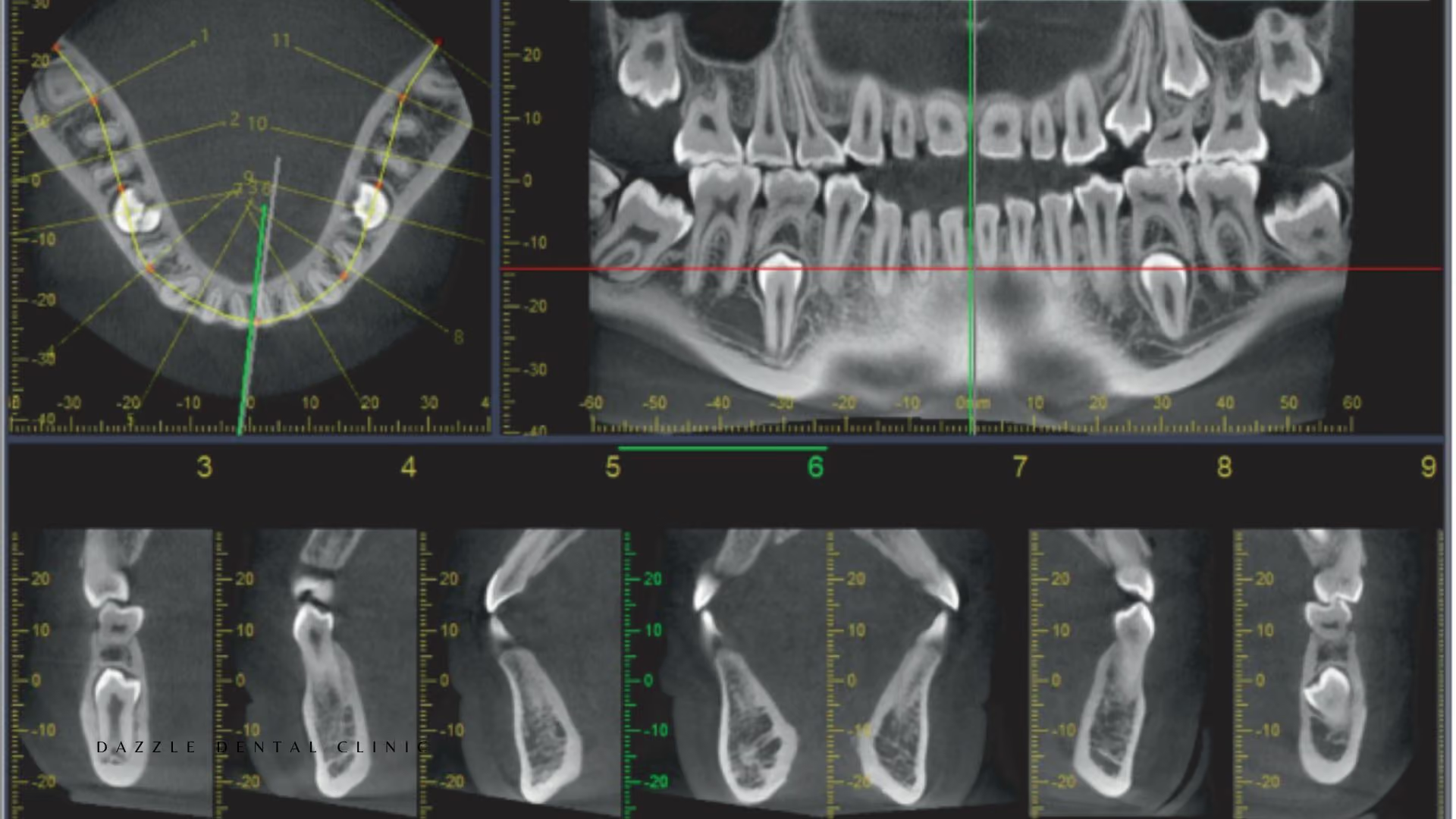
Cyst or pathology: A follicular cyst surrounding an impacted wisdom tooth, or other pathological changes identified on radiographic monitoring, require intervention. CBCT assessment of the relationship between the impacted tooth and the inferior alveolar nerve is essential for lower wisdom teeth where nerve proximity affects surgical planning.
When Extraction Is Not Necessary
Fully erupted, well-positioned wisdom teeth that can be cleaned and are not causing disease do not require extraction. Asymptomatic fully impacted wisdom teeth in patients over 35, where the risk of surgical complications increases with age, may be better managed with radiographic monitoring than prophylactic extraction.
The Surgical Procedure at Dazzle
Simple erupted wisdom tooth extraction: local anaesthesia, elevation of the tooth from the socket, sectioning if the roots are divergent or hooked. 15–30 minutes per tooth. Surgical removal of impacted wisdom teeth: local anaesthesia (IV sedation available for anxious patients or complex cases). A mucoperiosteal flap is elevated to expose the bone covering the impacted crown. Bone removal with a handpiece or piezoelectric instrument exposes the crown. The tooth is sectioned where necessary and removed. The socket is irrigated, the flap repositioned, and sutured. CBCT-guided planning is used for lower wisdom teeth where close proximity to the inferior alveolar nerve is identified.
Post-Operative Recovery
Swelling peaks at 48–72 hours and resolves over 5–7 days. Pain is managed with ibuprofen and paracetamol. Soft diet for 5–7 days. Gentle warm saline rinses from day 2. Dry socket (alveolar osteitis) occurs in approximately 5–10% of wisdom tooth extractions and is managed with socket irrigation and a medicated dressing at Dazzle.
FAQs
Q1: Do all four wisdom teeth need to come out at the same time?
No. Upper and lower wisdom teeth on the same side can be removed together; bilateral lower impacted extractions in the same appointment require more recovery management. The decision is based on clinical need and patient preference.
Q2: Is there a risk to the nerve from lower wisdom tooth extraction?
Temporary paresthesia occurs in approximately 1–8% of lower wisdom tooth extractions. Permanent paresthesia is considerably rarer (0.5–1%) and is more likely when the tooth apex is in very close contact with the nerve canal on CBCT.
Q3: What is coronectomy and when is it used?
Coronectomy is deliberate partial extraction — removing the crown of the impacted wisdom tooth while intentionally leaving the roots in place. Used when the CBCT shows the apex directly contacting or wrapping around the inferior alveolar nerve canal.
Q4: How do I prevent dry socket?
Do not smoke for at least 72 hours after extraction. Do not use a straw or rinse vigorously in the first 24 hours. After 24 hours, gentle warm saline rinses help keep the socket clean.


.avif)






